What Happens in a Psychoanalysis?
A View through the Lens of
The Analytic Process Scales (APS)
July 16, 2003
© 2003, Sherwood Waldron, Robert Scharf, David Hurst , Stephen Firestein & Anna Burton
Published in 2004, International. Journal of Psychoanalysis, 85: 443-466
Authors
Sherwood Waldron, M.D.
1235 Park Avenue, Suite 1B
New York, NY 10128
Tel: (212) 722-2248
Fax: (212) 410-6927
Email: sherwoodwaldron@post.harvard.edu
Robert D. Scharf, M.D.
207 East 74th Street
New York, NY 10021
Tel: (212) 988-4145
David Hurst, M.D.
601 Emerson Street
Denver, CO 80218
Tel: (303) 832-5024 Tel: (303) 832_5024
Stephen K. Firestein, M.D.
8 East 96th Street
New York, NY 10128
Tel: (212) 831-4554
Anna Burton, M.D.
163 Engle Street, Bldg. 2
Englewood, NJ 07631
Tel: (201) 567-4633
ABSTRACT
A group of experienced analysts has developed scales and a coding manual illustrated with clinical examples to evaluate recorded analyses and psychodynamic therapies. The Analytic Process Scales (APS) assesses three dimensions: (1) the contribution of the analyst: helping to develop a relationship in which the analyst can provide clarification and interpretation of transference and resistance; (2) the contribution of the patient: the communication of experience and the expression of feeling in ways which provide information about needs, wishes, and conflicts, accompanied by self-reflection; and 3) interactional characteristics of the emerging relationship, explored by studying sessions divided into psychoanalytically coherent segments.
A preliminary study of nine sessions has established that the variables assessed by the APS can be rated reliably. Study of the analyst’s contributions illuminated their varied and complex structure. Important differences emerged among the three patient-analyst pairs studied, and changes in scores over time tracked developments in the analytic work which would imply different treatment outcomes. The APS appears to be a reliable tool facilitating the systematic study of psychoanalyses.
[July 16, 2003 Text and endnotes 6,859 words, not including references or appendix].
BACKGROUND
There is a need for methods allowing systematic study of what happens in an analysis that do justice to the richness and subtlety of the work, and that permit evaluation of its varying quality. To demonstrate the efficacy of psychoanalytic treatment to those outside as well as within the analytic profession, and to improve treatment, we must identify and measure what happens in an analysis and ultimately correlate these measures with outcome (Waldron 1997a). With this in mind, a small group of experienced analysts in New York decided to develop the means to study tape-recorded psychoanalysis systematically, starting in 1985.
Our experiences had given us each the impression that when analysts assembled in small groups to discuss clinical work, substantial consensus developed over time. This impression stood in marked contrast to some research findings, epitomized in Seitz’s (1966) classic paper that reported no discernible consensus among psychoanalysts in evaluating psychoanalytic work. Our previous research experience also led us to anticipate a different result (Waldron et al., 1975; Waldron 1976).
Definitions of Psychoanalysis
Freud (1914, p.16) stated that any treatment based upon an understanding and application of the concepts of transference and resistance deserves to be called psychoanalysis. The continuing focus in the United States on the importance of addressing resistance was demonstrated by the results of five years of study of analytic process by the COPE study group of the American Psychoanalytic Association (Boesky 1990). This group accepted the centrality of Weinshel’s definition: “The resistance, together with its successful negotiation by the analyst (most often by interpretation), is the clinical unit of the psychoanalytic process” (1984, p. 69). Since the investigation and interpretation of a resistance usually results in illuminating some feature of the transference, Freud’s statement would appear still to be central to this conceptualization. But does this broad characterization capture the central aspects of observed psychoanalyses sufficiently? Systematic investigation is needed to determine what may differentiate psychoanalysis from other psychoanalytic psychotherapies in actual practice, and whether differences may prove to be best described quantitatively, rather than qualitatively..
In the last several decades, the previously clear theoretical distinctions between psychoanalysis and psychotherapy have crumbled to such an extent that Wallerstein (1995) describes a “World without Consensus” as his ninth chapter of The Talking Cures. In this comprehensive review, he cites various authors’ efforts to make distinctions based upon quantitative differences between psychoanalysis and psychoanalytic psychotherapy, an approach consistent with that of our research group. The findings of the Menninger Psychotherapy Research Project, studying 42 psychoanalyses and psychotherapies over a long period, support the view of a gradation of characteristics between the two treatments (Wallerstein 1986). Another description of the relationship between psychoanalysis and psychotherapy given by Thomä and Kächele is also consistent with our quantitative approach: psychoanalysis is psychotherapy with an “ongoing, temporally unlimited focal therapy with a changing focus” (1987, p.347). This “Ulm Process Model” reflects their view that the activities of both patient and analyst in treatments called psychoanalysis and psychotherapy can not be sharply differentiated, but that quantitative differences may exist. Kernberg also emphasizes quantitative differences, while stating that “any given session of psychoanalytic psychotherapy may be indistinguishable from a psychoanalytic session” (1999, p. 1080). However, he also states that the adherence to “technical neutrality” is what distinguishes psychoanalysis per se from psychoanalytic psychotherapy, a distinction meriting empirical investigation.
Theoretical Viewpoint of the Authors
If an individual psychotherapeutic process can be described in the most general terms as a meeting between two people in which one is expected to try to help the other with psychological problems, one feature of a psychoanalytic approach is the degree of attention paid to unconscious (in addition to conscious) elements as they are related to the patient’s suffering, whether these elements are intrapsychic conflicts, losses, pathologic defenses, or deficits in the development of the self, or of the functions of the ego or conscience.
Unconscious elements remain in their relatively inaccessible position because the suffering individual unconsciously resists awareness, with its anticipated danger of even greater suffering. Psychoanalysis has traditionally been conceptualized as attempting to lessen these obstacles to conscious awareness, examination, and problem solving, primarily by means of interpretation. However, more recent writings emphasize that the relationship with the analyst, a caring, knowledgeable, trusted person, fosters a sense of safety that decreases the apparent danger and need for defense (Sandler 1960, Levy & Inderbitzen 1997)..
The psychoanalyst encourages the patient to say everything that occurs to him or her. The limits of the patient’s awareness give early indication to the analyst of the patient’s core conflicts. From the beginning, the patient begins to feel known by the analyst, and through the analyst’s responses the patient begins to know him or her. Hopefully, the analyst becomes known as relatively non-judgmental, neutral, and abstinent of action, and the analysis becomes increasingly felt as a safer place to say what comes to mind. Self psychologists describe this part of the process, emphasizing empathic listening that allows selfobject transferences to develop (mirror, twinship and idealizing) (Kohut 1984 pp. 1982-193). In this atmosphere, the analyst attempts gradually to increase the patient’s access to unconscious elements by working with the obstacles that keep them outside awareness, the resistances or defenses. Psychoanalytic clinicians have observed that this process of growing awareness of what had been hidden is usually accompanied by progressive improvement in symptoms and greater freedom to experience feelings, relate to people and try new ways to live that were previously out of reach.
As improvement develops in other areas of the patient’s life, the patient’s suffering often becomes more alive in the here-and-now relationship with the analyst. This new locus of neurotic conflict, defense and inhibition may become the principal focus of the analytic work by patient and analyst as they attempt to experience and understand these central conflicts.
One would expect that beneficial change depends considerably on the quality of the analyst’s contributions, represented by the skill with which he or she finds the appropriate moment to intercede, the selection of type of analyst contribution and its content, and its articulateness. Attunement to the patient’s immediate focus, and coherence and continuity of the line of interpretation would also contribute to overall quality. Conversely, inappropriate, inept, untimely, even harmful approaches to resistances and transference manifestations would limit analytic progress (Gabbard et al. 1994).
For Freud (1923) a psychoanalytic approach addressed childhood sexuality and the Oedipus complex. In our systematic assessment we evaluate the clarification and interpretation of sex and aggression, since studies of recorded cases are needed to formally confirm or disconfirm the working hypotheses that addressing such matters is instrumental in therapeutic benefit. We also apply our rating scales to assess the degree to which both analyst and patient address development, seeking an empirical basis for evaluating the role of reconstruction.
Traditional psychoanalytic technique proscribed answering questions directly, being self revealing, and making supportive analyst contributions. Abend’s (1990) definition of analytic process includes these kinds of proscriptions in his sixth criterion: “utilization of a framework for treatment, called the analytic situation, that firmly restricts the means by which the analyst seeks to influence the patient” (p. 539; emphasis ours). Whether such proscriptions lead to freer association, better self-reflection, or greater general improvement has not been empirically established. By approaching data by methods such as the APS, a systematic examination can be made about the relationship of such technical elements to the benefit derived.
Previous empirical studies
Despite efforts to describe the characteristics that make psychotherapy psychoanalytic, there are few empirical studies. Vaughan et al. (1997) developed a scale, the Columbia Analytic Process Scale or CAPS, for evaluating psychoanalytic process. It had three elements: the presence of free association (a patient variable), of interpretation (an analyst variable), and of working through (another patient variable). The latter was considered present if a patient demonstrated “insight or understanding” about the self, fantasy, transference, or genetic history. In studying sixteen sessions from nine patients, interrater reliability between two of the authors was modest but significant (Kappa of .5). They next attempted to establish the validity of the CAPS by comparing its results to the evaluations of 10 experienced analysts as to whether analytic process was present in five of these sixteen sessions. Each rater was instructed to use his or her own definition, based upon only one session from each case. The results were disappointing and the authors concluded that “there is no meaningful consensual definition of the term” (p. 964). However, there are good reasons to view the limited results as reflecting specific methodological limitations, most notably the study of only one session and the lack of advance definition of terms (Waldron, 1997b).
The studies of Enrico Jones and collaborators (Jones & Windholz 1990, Jones & Pulos 1993, Ablon & Jones, 1998, Albani et al. 2002) have successfully characterized features of psychoanalytic process. Their Psychotherapy Process Q-Set (PQS) identifies dimensions of psychoanalytic process evident within a session as a whole. The PQS does not rate the within-session interactive process of patient and analyst, a feature that limits its ability to evaluate the immediate effects of analytic contribution.
In addition to the PQS, there are several other instruments that have been applied to recorded analyses, such as Luborsky’s Core Conflictual Relationship Theme (CCRT) (1990); the Psychodynamic Intervention Rating Scale (PIRS) developed by Cooper and Bond (1998), which has been used to assess relationships between process and outcome in brief therapies (Milbrath et al. 1999); the Vanderbilt Psychotherapy Process Scales or VPPS (O’Malley, Suh and Strupp 1986); and the Therapist Verbal Intervention Inventory or TVII (Koenigsberg et al,1988, 1993). Bucci (1997) applied her linguistic measure of Computerized Referential Activity and the linguistic measures for Emotion Tone, and Abstract Expression developed by Mergenthaler to the recorded case of Mrs. C, as an illustration of a model of psychoanalytic process which she calls the referential cycle The patterns of this cycle, along with inspection of the content of sessions, are seen as reflecting the degree to which the analyst contributions led to a deepening of the analytic work.
A definition of psychoanalytic process combining clinical breadth with scientific clarity has not been available. Compton (1990) and Boesky (1990), both participants in the COPE study group, have called for further empirical studies as the direction for future efforts in investigating psychoanalytic processes. The APS builds on these previous measures by bringing together in a succinct way a multi-faceted assessment of the functioning of analyst and patient from a clinical psychoanalytic point of view, with assessment of analyst contribution quality, as will be seen below.
HOW THE APS SCALES WERE DEVELOPED
The goal of our research group has been to examine the changes occurring over time in various psychoanalytic treatments, and what features of the work of patient and analyst account for these changes. We expect to find quantitative, rather than qualitative differences between psychoanalysis and psychotherapy. We anticipated that juxtaposing systematically gathered data with clinical qualitative descriptions would provide the richest opportunity to integrate psychoanalytic understanding with empirical methods, as was accomplished in the careful study of Jones and Windholz (1990).
Our group set out 18 years ago to develop methods for systematic assessment of analytic process based on clinical understanding. We understood that our theoretical training would influence how we viewed the key components of treatment, but we attempted to lessen this influence by using a “bottom up” procedure, listening to tape recorded psychoanalytic sessions, and discussing our specific clinical understandings of the material. Several years of meetings once or twice monthly were spent studying sessions from six patients available to us through the Psychoanalytic Research Consortium. We each described what elements in a given session seemed relevant to understanding the contributions of both parties to the evolving treatment.
At first our group had differing impressions when listening to the same analytic hour, as had been previously reported in the literature (e.g., Seitz 1966). We discovered that studying two or three sessions immediately preceding the sample to be rated led to much greater agreement. The need for a substantial context in studies of psychoanalysis and psychotherapy has been mentioned by Mintz and Luborsky(1971), Schaffer(1983), and Messer et al(1992).
The next step was to formulate a description of each relevant dimension and rate the degree to which we felt each characteristic was present in the material of the session. For this purpose, we used a five-point Likert-type scale. The “0” point of the scale represented the absence of the characteristic, and the “4” point of the scale its strong presence, with the other points in-between. Each such description became one of our variables for describing the contributions of analyst or patient. In the course of our work, we defined our variables in simple, direct clinical terms as free of theory, ambiguity, and controversy as possible, and we specified that raters anchor their ratings in observable data.
Next we developed the APS Coding Manual, which describes a clinical situation anchoring the scale points of each variable. Over several years, we repeatedly modified this manual based upon our experience scoring new sessions while referring to the definitions and examples in the Coding Manual. Some variables were discarded because they could not be rated reliably, and new variables were added when we identified an important previously unrated dimension of the process. All the variable definitions and examples were progressively modified based upon ongoing experience and discussion of scoring discrepancies. This process ultimately yielded a set of 14 patient variables and 18 analyst variables described further below.
Dividing a Session into Clinically Meaningful Segments
From the beginning, we observed the utility of focusing our observations on serial units of the session being studied. Dividing a session into clinically meaningful segments provided us a means to examine the influence of each participant on the other in the course of each session. Our procedure for segmenting was a modification of that described by Stinson, et al. (1994). The division into segments is often at the point of a change in speaker resulting in analyst segments and patient segments. When there is a rapid exchange between patient and analyst a segment may include several changes of speaker and is rated for both analyst and patient variables. The interaction between analyst and patient is studied by looking at the relationships between the patient and analyst variables studied over time. The segmenting procedure usually leads to about 8 to 30 segments per session.
Using our segmenting manual illustrated by clinical examples, psychoanalytically informed clinicians can segment sessions with substantial agreement. Two advanced psychology students, both experienced in psychoanalytic research, segmented 23 sessions from two analytic cases. The segmenters were instructed to keep the raters’ task in mind and were trained as APS raters to maximize their appreciation of what constitutes a useful segment for our purposes. We found that, of 578 turns of speech which could have been chosen as a segment boundary, 95% of the time there was a perfect match between one segmenter and the other as to whether a given boundary was chosen (see Appendix, Table 1. For the statistically inclined, Cohen’s Kappa was .86). These results establish the reliability of the segmenting procedure in our hands.
The discovery that clinicians agree as to what constitutes a meaningful unit of analytic work is consistent with our view that it is feasible to develop appropriate methodologies for the assessment of psychoanalytic work. It may also often correspond to what the Boston Change Process Study Group (Nahum et al. 2002) describes as a relational move – what they label as the smallest slice of verbal or non-verbal action that could be parsed as an intersubjective intention (p. 1058).
THE APS VARIABLES, WITH AN ILLUSTRATION
We apply our 18 analyst variables and/or our 14 patient variables to sequential respective segments of recorded psychoanalytic sessions. APS raters evaluate each new segment in the context of previous segments, but are kept blind to the future segments of the session, and can not change their previous ratings based upon subsequent developments in the material.
In the sections to follow, we describe the variables that we have developed. We rate the degree to which each relevant aspect of psychoanalytic process (each analyst or patient variable) was present in each relevant segment.
Variables Rating Psychoanalytic Activities of the Analyst
We may define a psychoanalytic process, from the vantage point of the analyst, as a psychotherapeutic situation in which the therapist-analyst intervenes with clarification and interpretation of the patient’s conflicts, particularly addressing defense (resistance), and conflicts related to the analyst or analytic situation. The analyst addresses conflicts about sex and aggression, often includes a developmental dimension, and uses skill and attunement in approaching the patient’s states of mind . The analytic process is further facilitated by the analyst’s understanding of his or her own responses and by negotiating his or her own resistance through self reflection. To investigate systematically these features, based upon our clinical experience and the readings cited above, we derived four aspects of activities of the analyst:
Variables assessing the type of analyst contribution, including the degree to which the analyst clarifies, interprets, encourages elaboration, or provides support in the segment being rated;Variables assessing the aim of the analyst contribution in the segment, including the degree to which the analyst addresses defenses (resistances), transference, and the patient conflicts. Also rated are the degree to which the analyst contribution addresses romantic or sexual matters, problems with assertiveness, aggressiveness or hostility, issues involving self-esteem, and manifests a developmental focus;
Variables assessing analyst involvement: degree to which the analyst is confrontational, and demonstrates amicable or hostile feelings towards the patient;
Variables assessing the quality of the analyst’s contribution, including the degree to which the analyst follows the patient immediate emotional focus, intervenes in a way which shows psychological continuity with previous analyst contributions, is apt in content, timely and tactful, and is presented with psychological appeal to the patient.
We consider five of these analyst contribution variables as constituting core analytic activities: two types of analyst contribution, interpretation and clarification, and three aims of the analyst contribution, addressing transference, resistance, and other aspects of conflict.
The raters estimate the degree to which each of these core analytic activities is present, specifically disregarding the aptness or skill with which they are employed (since the quality of each analyst contribution is assessed separately via our “quality” variables). Each of these five elements is rated independently of the others, so that, for example, a given analyst contribution could be rated “4” for clarification, “2” for interpretation, “2” for addressing transference, “1” for addressing resistance and “0” for addressing conflict. The core analytic activities are further defined as follows:
Clarification is rated by the degree to which attention is called to insufficiently noticed surface features and how they may be psychologically connected, often by presenting several features as related to one another.
Interpretation is rated according to the degree to which the analyst’s contribution transforms meaning by bringing aspects outside of awareness into full awareness.
Addressing resistance is rated as the degree of focus on any measure the patient takes to avoid experiencing objectionable impulses, affects, thoughts, or fantasies (including, for example, compliance as a resistance, see Stein 1981). We use the term resistance because it is a well-known term, but we prefer our definition: “defenses in action during this segment.” Resistance may simultaneously serve drive, moral, or adaptive purposes. Addressing resistance must be manifest or, if inferred, easily identifiable in order to be scored. Raters evaluate the apparent aim of the analyst contribution, not whether defenses are actually present in the patient’s communication, or the skill with which they are addressed.
Addressing transference is rated according to the degree to which the patient’s reactions to the analyst or to the analytic situation are pointed out. The score increases as the analyst contribution is more direct, complex, and elaborated.
Addressing conflicts is rated according to the degree to which the analyst focuses on aspects of the patient’s conflicts in the segment – impulses or affects, their feared consequences or moral concerns, and the connections between any of these, including related fantasies and memories.
The following example of an analyst contribution illustrates the kinds of results generated by applying the APS. In the last day of a patient’s analysis, he had indicated a reluctance to talk, and expressed the fantasy of leaving early since he felt there wasn’t that much to say. Meanwhile, in the previous session, in discussing his fear of abandonment, he had remembered a photograph of his mother holding him at arm’s length, as if (he felt) she were experiencing distaste at this infant and his needs. He wondered if the analyst would say anything if he got up to leave. The analyst replied:
T: “Think where we ended yesterday . . . with the most dramatic, image. Today is like a continuing elaboration of it except that you’re not consciously aware of it. I remind you of the photograph of your mother holding you at arms’ length. That’s exactly what you’re experiencing with me today, but also creating with me saying, “listen, I don’t want to talk to you. I don’t want to be involved with you today. I’m uncomfortable here. I don’t want to relate to you” is what you are saying to me and also what you expected from me.
P: mm-hmm
T: and by the way, that was immediately after you had dared to violate the ‘arms length’ rule, after you had dared to say, “look, I might very well want to call you. Would that be something you would welcome?” and I had said “yes.” (from patient “U8”, described later. With permission from the patient, through the Psychoanalytic Research Consortium.)
The following scores for core analytic activities on this segment were obtained by averaging the scores of four raters. Recall that each variable is rated on a five-point scale, extending from “0” to “4” for the degree to which the segment fitted each of the variable definitions. This analyst’s contribution was viewed as an interpretation (score 2.75 out of a maximum of 4), but also as a clarification (2.25 out of 4). It was rated as addressing transference strongly (3.5 out of 4), and addressing defenses manifest in the session (2.75 out of 4). Since the analyst did not spell out how the patient was in conflict about closeness and neediness, although he addressed the elements of the patient’s conflict, the score for addressing conflict was only 1.5 out of 4 possible. In this segment the raters felt the analyst was following the patient well (3.0) and that the analyst contribution overall was of high quality (3.0).
Variables Rating Psychoanalytic Activities of the Patient
In order for the analyst to develop an understanding of the patient, which may lead to clarifying and interpreting activities, the patient associations must convey inner experiences which permit the analyst to perceive and understand her conflicts. The degree to which the patient conveys her experience of the analyst and analytic situation (transference) is rated separately from her experience outside the analytic situation, and each area is rated for the degree to which the patient shows self reflection. While communicating experiences, patients vary in the degree to which their expressed feelings contribute to understanding, which we rate as well (requiring listening to the tape recording).
We can summarize here that a patient contributes to a psychoanalytic process insofar as s/he conveys experiences in ways which provide opportunities for the analyst to understand her conflicts; and insofar as the patient reflects upon her experiences and expresses feelings in ways which enhance her own and the analyst understanding of her conflicts. The relationships among self-reflection (Busch 1994), self-observation, self-inquiry (Gardner 1983) self analysis (Calder 1980), and insight (Kris 1956, Hatcher 1973, Horowitz 1987, Abend 1988) is important but will not be discussed further here.
Rating the Interaction
As we appraise the degree to which psychoanalytic work is taking place in the psychoanalytic (psychotherapeutic) situation, we determine the characteristically psychoanalytic features of the analyst contribution, of the patient contribution, and their interaction. Most current authors emphasize the importance of the interaction (Levine 1994, Burland 1997, Boesky 1998). By psychoanalytic interaction we hope to find a mutual spiraling potentiation of understanding, with the analyst remarks leading to the development of further patient material and self reflection, and the patient remarks providing an opportunity for the analyst to add to further understanding in an evolving process (Schlesinger 1974). The interaction undoubtedly affects both patient and analyst in a wide variety of other ways as well.
Additionally, assessing the degree to which psychoanalytic work is taking place is augmented by a longitudinal perspective, comparing the work at different points in the treatment. Psychoanalyst evaluators can confirm longer-term progress, or see that patient psychoanalytic work is not progressing (Stein 1981). As Boesky (1990) and Weinshel (1990) have pointed out, process as a term derives from the word for progress, motion forward. Accordingly the psychoanalytic process should be evaluated as to progress leading to a reduction of the patient suffering and disability, and the enhancement of positive aspects of mental health. This outcome aspect of the work of the APS group is not reported in this paper, but constitutes one aspect of our ongoing efforts.
FACE VALIDITY OF THE APS
In evaluating what happens in a psychoanalysis, our group has developed scales that closely track the clinical data of each segment of the analytic session, drawing upon our clinical experience and previous psychoanalytic and psychotherapy research to formulate our variables. We have also had the benefit of suggestions from many clinicians with whom we have discussed our work both informally and in presentations in a wide variety of settings. The validity of the APS depends on how well we have captured dimensions that clinicians consider important. Each clinician reader may compare the variables and definitions given in our Coding Manual (see endnote 5) with their own understanding of clinical work to develop their own opinion of the validity of our measuring instrument.
There can be no doubt that the perspectives of the authors limit the scope of the Analytic Process Scales (APS). Viewpoints of analysts from Latin America and Europe will undoubtedly enrich the APS and its manual, at such time as colleagues from these places may choose to work with or add items to our Coding Manual.
RELIABILITY OF THE APS
Central to the potential usefulness of our research instrument is its inter-rater reliability. Using the APS Coding Manual, both inexperienced and experienced clinicians have been able to achieve reliability simply on the basis of careful study of the Coding Manual as they carry out their ratings. These figures are shown in Tables 1 and 2 of the Appendix. They provide the reader with an opportunity to study the variety of variables rated, as well as to examine the general level of reliability of our ratings.
The experienced psychoanalyst raters who carried out the examination of the three patients reported below and in our following paper (Waldron et. al 2003) achieved the highest reliability, reflecting their experience as clinicians and their experience in using the APS (three columns furthest to the right).
The inexperienced clinician raters initially had difficulty assessing the patients’ analytic productivity, and assessing the quality of the analyst’s contributions (line 1, table 1 and lines 1 & 2, table 2). This would be expected, since these dimensions are the most difficult to rate. The inexperienced clinicians’ reliability on these more difficult-to-rate variables approached or exceeded that of the experienced raters with additional teaching about psychodynamic therapy and additional experience making ratings. Furthermore, the inexperienced raters’ scores on most of the other variables are approximately comparable to the experienced raters.
UTILITY OF THE APS ILLUSTRATED: EVALUATING THREE CASES
Scores from a preliminary sample studied using the APS provide an illustration of the utility of the instrument. Three treatments were drawn from a database of eighteen analytic patients then in the collection of the Psychoanalytic Research Consortium (described and referenced above). The cases were selected initially in order to develop and test our scales, on the basis of three criteria: 1) we sought three different analysts to give more breadth to the sample; 2) we chose cases which on clinical inspection showed a variety of courses and outcomes; 3) we wished to minimize the number of cases studied in this early phase, so that we would have more fresh cases for our later researches into the relationship between process and outcome. For the first two cases described below, the sessions were chosen from the very beginning, the middle, and a few weeks before the end of the treatment, with no other selection criteria except that the sessions were from a complete week of analytic work. The third case described below was chosen in accordance with criterion 3 above, because it was only recorded at the end of analysis, hence was not suitable for later study of change in the course of treatment, since there were no recordings available of early sessions. Raters were not given any summary of the case beforehand, nor were they privy to the judgment by the senior author as to the quality of the work until after doing their ratings.
One patient had done relatively well; another appeared to be deadlocked and ended after 660 sessions; the third analysis was chosen as a good representative of analytic process. Although we make no claim that the sample is representative of all analyses, there were no systematic biases in selecting these cases. Of course, only patients who had agreed to be audiotaped could be included.
Patient A2 was a young agoraphobic housewife and mother whose symptoms improved considerably in the course of her three-hundred-hour-plus, four times weekly analysis, which became a twice-weekly treatment as termination approached. Despite her improvement, her analyst thought she would have benefited from further work. Our raters concurred. Generally, they thought that the analyst-patient interaction was negatively influenced by this male analyst’s imposing presence, towards which the patient seemed unusually compliant. They also thought that the analyst emphasized transference analysis in ways that were often not meaningful or useful to the patient. Despite this, the analyst seemed sensitive and attuned to the patient in ways that she appreciated and responded to positively.
Patient U8 was a married man experiencing relationship problems who had left a previous analysis because he felt too distant from the analyst. The present two-year analysis with another male analyst (about 400 hours, four times weekly) addressed how he kept himself removed from others, including spouse, children, and his present and previous analyst. It resulted in positive changes in both his analysis and his life. His analyst’s contributions aimed at conflict and defense, and he was unusually active. This analysis was seen as a partially successful effort to break through the patient’s wall of isolation and passivity.
Patient V4 had serious difficulties in relationships including distancing himself from women. His initially positive reaction to this, his second, male analyst gradually gave way to a sense of alienation and feelings of being misunderstood. The analyst became increasingly frustrated and appeared to blame the patient for his failing marriage and faltering treatment, which ended after 660 hours. The analyst was rated as very confrontational and emotionally expressive. The confrontations seemed to become increasingly hostile. An absence of effective or meaningful interpretations of the pair’s antagonistic relationship may have undermined the possibility of more productive analytic work.
Figure 1 (Appendix) shows the APS Core Analytic Activities scores from our sample of 123 analyst segments from 9 psychoanalytic sessions of these three patient-analyst pairs. The horizontal axis shows the levels of core analytic activities (clarification, interpretation, addressing resistance, addressing transference, and addressing conflict) for each case. The vertical axis shows the percent of analyst segments in which each of the core analytic activities appears substantially.
The APS profiles each treatment, showing the analysts’ use of the five core analytic activities, and the differences between them. All three address transference frequently (88% of analyst contributions for U8, 78% for A2 and 40% for V4 had a substantial component of addressing transference).. But only two analysts use a substantial percentage of clarification and
interpretation (A2 and U8), and approach the patients’ conflicts and defenses/resistance (64% of the analyst contributions for U8 had a substantial component of addressing defenses, compared to 28% `for A2 and none for V4 ). In other words, this application of the APS suggests that there was much more analytic process present (by our definition) in those two cases than in the third. The striking differences in addressing conflicts and defenses demonstrate in this small sample the variability of analysts’ work. These differences in core analytic activities among the analysts are statistically significant (Figure 1 asterisks). We find that almost all the levels of core analytic activities were different for each of the three analyses.
The APS provides a systematic description of the complex nature of analyst contributions. Figure 2 (Appendix) shows the results of rating analyst contributions as to the degree to which they conformed with each of our four “types.” Each bar is composed of those interventions (segments) receiving the highest score for that type of analyst contribution. Recall that a single analyst contribution might be rated “4” for clarification, “2” for interpretation and “1” for support, and “0” for encouraging elaboration, for example. In the figure, the length of each bar indicates the relative frequency that each type of analyst contribution led the others by segment. It may be seen that interpretation was the most frequent leading analyst contribution, followed closely by clarification and encouragement to elaborate. Support accounted for only seven percent of the analyst contributions. This distribution overall shows that the work of the three analysts is largely analytic in nature.
The shadings within each bar show the degree to which these analyst contributions are relatively “pure” in type (the leftmost shaded area for each bar), with the other parts of the bar representing the mixtures found in this sample. The majority of analyst contributions were mixed. About half the interpretations were combined with clarification; two-thirds of clarifications were mixed with other types, half of these being simultaneously classified as
interpretations and the other half in other combinations. We found that the interpretations which were combined with clarification received a higher rating for quality than interpretations given without a clarifying component (t-test significant at the .015 level). This preliminary finding might suggest that sharing the basis for one’s interpretation (the clarifying component) enhances the quality of an interpretation. Supportive elements rarely appeared in pure form, but were usually alloyed with the other types, and encouragement to elaborate was least often mixed with other elements of analyst contribution, as might be expected clinically. Five percent of the analyst contributions were of a sufficiently mixed nature that they received scores on all four types of analyst contribution.
The study of analyst contribution types generated a hypothesis that analyst contributions which clearly can be classified on the APS indicate higher quality work by the analyst. We anticipated that a clearly framed analyst contribution would receive at least a score between “1″ and “2″ (1.5 or better) for at least one type of analyst contribution. We found that the three analyses differed in this respect. In the treatment that seemed to be going the best (U8) a large proportion of the analyst’s analyst contributions (two-thirds) fit at least one type. The next best treatment (A2) had about half the analyst contributions fitting this definition of a type. But V4, the case which was judged as least successful by other criteria, had less than 10% of the analyst contributions fitting a type. So, in this small sample, the typing of analyst contributions on the APS not only characterizes the nature of the analytic activity, but offers an indication of the quality of analyst contributions, with poorer work being apparently harder to characterize.
The APS clearly evaluated the analytic contribution of each patient, and differentiated between patients (Figure 3, Appendix). There were substantial differences in patient participation among the three cases. Both the A2 and the U8 patient surpassed the V4 patient on all six variables. Three of the variables also showed minor differences between A2 and U8 as well. In the figure, the asterisk on top of each bar indicates that that bar was statistically significantly different from the others. These differences appear to verify the clinical impressions of the raters, as described in the short case vignettes above.
The APS was able to show significant changes in the patients’ contribution from one point in the analysis to another. Patient A2’s functioning improved significantly from early to late in her analysis in conveying experience (related to free association), and in experiencing her own attitudes as problematic. Also the quality of her contributions became significantly higher compared to the early period in the analysis. In contrast, patient V4 showed a significant decline from early to late in these same variables. Thus the APS may be used for studying changes in the quality of the ongoing treatment process during the analysis. Further study may demonstrate a correlation of changes in such “within-session outcome measures” with independently derived measures of outcome (Waldron1997a).
The APS interaction variables also differentiated among the three cases. Both the degree to which the analyst followed the patient and the patient’s responsiveness to analyst contributions were significantly different among the patient-analyst pairs. These differential interaction patterns confirmed our global clinical impressions of the cases. With the APS, we hope to explore systematically the mutual influence of the patient’s and analyst’s contributions to the ongoing process. This is reported in further detail in our subsequent paper (Waldron et al. 2003).
DISCUSSION
The authors have developed a tool, the Analytic Process Scales, which provides a measure of what happens in psychoanalysis and psychoanalytic psychotherapy. We report its application to three recorded analyses, measuring the degree to which the patients participated meaningfully in the analytic process and the degree to which the analysts used core analytic activities (such as clarification and interpretation) skillfully. Additional methodological refinement is needed to establish further the psychometric properties of the APS, for example by clarifying the impact of rater theoretical orientation, and establishing convergent validity by correlating APS scores with other sources of information. Nevertheless our preliminary study suggests that the APS may provide a useful measure of analyst contribution quality, patient productivity, and bi-directional interactional influence. The description of the activity of these analyst-patient pairs is succinct, systematic, and directly reflects clinical psychoanalytic thinking. The reliabilities we have found using a variety of raters on this material suggests that other investigators could use our methodology reliably.
The large differences in levels of psychoanalytic activity we found between the three analysts in this sample may indicate clinically significant distinctions between the treatments. To know whether these findings are significant for each case, we need to measure how consistently they appear in other sessions of the same patients, and we require follow-up data on the results after treatment ended.
Our findings show the complexity and overlapping nature of contributions by the analyst, giving further support for the need to assess psychoanalytic work using continuous variables, in preference to either/or variables such as: “was this intervention an interpretation or not?” or “was analytic process present in this session?” Such dichotomous variables are unlikely to justly characterize psychoanalytic treatments.
Systematic examination of what happens in the analyst-patient interaction is perhaps the most promising direction for psychoanalytic research. Approaches such as the APS facilitate quantitative studies of clinical variables in psychoanalytic and psychotherapeutic work, which can be integrated with complementary qualitative examination of the contributions by both parties to the clinical situation (Jones 1990; Stiles 1993). A number of hypotheses about what happens in psychoanalysis, and how each participant influences the other, can be tested, based upon examining the sequences of APS scores. This may further our understanding of analytic process and suggest improvements in technique. Investigating such hypotheses may be more likely to lead to advances in technique and the understanding of analytic process than discussion based on clinical vignettes. Methods for evaluating sequential developments in psychoanalytic work provide the opportunity to support or disconfirm presumed causal relationships (Gassner et al. 1982; Elliott 1991; Milbrath et al. 1999; Crouse et al. 2003), which is important for scientific progress.
In summary, current developments in psychoanalytic process research have furthered the possibility of assessing the complex relationships occurring between patients and analysts to determine what changes in patients occur in conjunction with what elements present in a psychoanalysis or psychoanalytic psychotherapy (Waldron 1997a, Waldron et al. 1998). The authors are undertaking further studies to determine the stability and fluctuation of APS scores during any phase of treatment, as well as developing “within-session” measures of outcome in addition to the APS, in order to link our measures of process with independent psychological measures of outcome at the end of treatment and thereafter (Leuzinger-Bohleber et al., 2003). Such studies hold the promise of greatly strengthening the empirical basis of psychoanalytic work.
REFERENCES
Abend S (1988). Neglected classics: Ernst Kris’s “On some vicissitudes of insight in psychoanalysis.” Psychoanal. Q., 57:224-228.
Abend S (1990). The psychoanalytic process: motives and obstacles in the search for clarification. Psychoanal. Q., 59:532-549.
Ablon J & Jones EE (1998). How expert clinicians’ prototypes of an ideal treatment correlate with outcome in psychodynamic and cognitive-behavioral therapy. Psychotherapy Research, 8: 71-83.
Albani C, Blaser G, Jacobs U, Jones E, Thomä H & Kächele H (2002). Amalia X psychoanalytic therapy in the light of Jones Psychotherapy Process Q-Sort. In: Leuzinger-Bohleber, M., Traget, M. (Eds.) Outcomes of Psychoanalytic Treatments: Perspectives for Therapists and Researchers. Whurr Publishers, London & Philadelphia, 294-302.
Boesky D (1990). The psychoanalytic process and its components. Psychoanal. Q., 59:550-584.
Boesky D (1998). Clinical evidence and multiple models: new responsibilities. J. Amer. Psychoanal. Assn., 46:1013-1020.
Bucci W (1997). Patterns of discourse in good and troubled hours: a multiple code interpretation. J. Amer. Psychoanal. Assn., 45:155-187
Burland J (1997). The role of working through in bringing about psychoanalytic change. Int. J. Psycho-Anal., 78:469-484.
Busch F (1994). Some ambiguities in the method of free association and their implications for technique. J. Amer. Psychoanal. Assn., 42:363-384.
Calder K (1980). An analyst’s self-analysis. J. Amer. Psychoanal. Assn., 28:5-20.
Compton A (1988). COPE Study Group Discussion of the Psychoanalytic Process Unpublished.
Compton A (1990). Psychoanalytic process. Psychoanal. Q., 59:585-598.
Cooper S & Bond M. (1998). The Psychodynamic Intervention Rating Scale. Unpublished.
Crouse, J., Burton, A., Firestein, S., Scharf, R., & Waldron, S. (2003). A path analytic strategy to analyze psychoanalytic treatment effects. Int. J. Psychoanal.84:1263-1280.
Elliott R (1991). Five dimensions of therapy process. Psychotherapy Research, 1:92-103.
Freud S (1914). On the History of the Psycho-analytic Movement S. E. 14.
Freud S (1923). Two Encyclopaedia Articles. S. E. 18.
Gabbard GO, Horwitz L, Allen JG et al. (1994) Transference interpretation in the psychotherapy of borderline patients: a high risk, high gain phenomenon. Harvard Review of Psychiatry 4: 59-69.
Gardner M R (1983). Self Inquiry. Boston: Little Brown.
Gassner S, Sampson H, Weiss J & Brumer S (1982). The emergence of warded-off contents. Psychoanalysis and Contemporary Thought, 5:55-75.
Hatcher, R (1973) Insight and Self-Observation. J. Amer. Psychoanal. Assn., 21:377-398
Horowitz M (1987). Some notes on insight and its failures. Psychoanal. Q., 56:177-196.
Jones EE & Windholz M (1990). The psychoanalytic case study: toward a method for systematic inquiry. J. Amer. Psychoanal. Assn., 38:985-1015.
Jones EE & Pulos SM (1993). Comparing the process in psychodynamic and cognitive behavioral therapies. Journal of Consulting and Clinical Psychology 61: 306-316.
Kernberg OF (1999). Psychoanalysis, psychoanalytic psychotherapy and supportive psychotherapy: contemporary controversies. International Journal of Psychoanalysis, 80: 1075-1091.
Koenigsberg H, Kernberg O, Rockland L et al. (1988). Developing an instrument for characterizing psychotherapy techniques in studies of the psychotherapy of borderline patients. Psychoanalytic Process Research Strategies. ed. H. Dahl, H. Kaechele, & H. Thomae New York: Springer-Verlag, 147-162.
Kohut H (1984). The role of empathy in psychoanalytic cure. In Kohut, H. How Does Analysis Cure? A. Goldberg (Ed.), Chicago, University of Chicago Press.
Kris, E. (1956) On Some Vicissitudes of Insight in Psycho-Analysis. Int. J. Psycho-Anal., 37:445-455
Leuzinger-Bohleber M, Stuhr U, Ruger B & Beutel M (2003). How to study the ‘quality of psychoanalytic treatments’ and their long-term effects on patients’ well-being: a representative, multi-perspective follow-up study. International Journal of Psychoanalysis, 84: 263-290.
Levine H (1994). The analyst participation in the analytic process. Int. J. Psycho-Anal., 75:665-676.
Levy S and Inderbitzin L (1997) Safety, danger, and the analyst’s authority. Journal of the American Psychoanalytic Association., 45:377_394.
Luborsky L & Crits-Christoph P (1990). Understanding Transference: the CCRT Method. New York: Basic Books.
Messer S, Tishby O & Spillman A (1992). Taking context seriously in psychotherapy research: relating therapist interventions to patient progress in brief psychodynamic therapy. Jour. Cons. Clinical Psychol., 60:678-688.
Milbrath C, Bond M, Cooper S, Znoj HJ, Horowitz MJ & Perry JC (1999). Sequential consequences of therapists’ interventions. Journal of Psychotherapy Practice & Research, 8: 40-54.
Mintz J & Luborsky L (1971). Segments versus whole sessions: which is the better unit for psychotherapy process research? Jour. Abnormal Psychol., 78: l80-l9l.
Nahum JP for the The Boston Change Process Study Group (CPSG) Brushweiler-Stern N, Harrison AM, Lyons-Ruth K, Morgan AC, Nahum JP, Sander L W, Stern DN & Tronick EZ (2002). Explicating the implicit: The local level and the microprocess of change in the analytic situation. International Journal of Psychoanalysis, 83: 1051-1062.
Sandler J (1960) The background of safety. Int. J. Psycho_Anal., 41:352_356
Schaffer N (1983). The context of therapist behavior and outcome prediction. Professional Psychology: Research and Practice, 14:656-669.
Schlesinger H (1974). Problems of doing research on the therapeutic process in psychoanalysis. Jour. Amer. Psychoanal. Assoc, 22:3-13.
Seitz P (1966). The consensus problem in psychoanalytic research. Methods of Research in Psychotherapy. Gottschalk, L. & Auerbach, A. H. (eds.). New York: Appleton-Century-Crofts.
Stein, M H (1981). The unobjectionable part of the transference. Jour. Amer. Psychoanal. Assoc., 29: 869-892.
Stiles, WB (1993). Quality control in qualitative research. Clinical Psychology Review, 13: 593-618.
Stinson C, Milbrath C, Reidbord S & Bucci W (1994). Thematic segmentation of psychotherapy transcripts for convergent analyses. Psychotherapy 31: 36-48.
Suh, CS, Strupp, HH, and O’Malley, SS (1986) The Vanderbilt Process Measures: The Psychotherapy Process Scale (VPPS) and the Negative Indicators Scale (VNIS). In Greenberg, L.S. & Pinsof, W.M.(Eds.) The Psychotherapy Process: A Research Handbook (pp. 285-323). New York, Guilford Press.
Thomä H & Kächele H (1987) Psychoanalytic Practice 1: Principles. Springer-Verlag, New York.
Vaughan S, Spitzer R, Davies M & Roose, S. (1997). The definition and assessment of analytic rocess: Can analysts agree?. Int. J. Psycho-Anal., 78:959-973
Waldron S (1976). The Significance of Childhood Neurosis for Adult Mental Health: A Follow-Up Study. American Journal of Psychiatry 133:532-538.
Waldron S (1997a). How can we study the efficacy of psychoanalysis? The Psychoanalytic Quarterly, 66:283-324.
Waldron S (1997b) Discussion of he Columbia Psychoanalytic Process Scales (Research in Progress Meeting, American Psychoanalytic Association, Midwinter Meetings, New York. available at http://www.psychoanalyticresearch.org.
Waldron S, Scharf RD & Firestein SK (1998). Introduction for colleagues to the analytic process scales. Available at http://www.psychoanalyticresearch.org.
Waldron S, Scharf R, Crouse J, Firestein S, Burton A & Hurst D (2003). Saying the right thing at the right time as judged by The Analytic Process Scales (APS). Psychoanal. Q.., in press.
Waldron S, Shrier DK, Stone B and Tobin F (1975): School phobia and other childhood neuroses: A systematic study of the children and their families. American Journal of Psychiatry l32: pp. 802-808.
Wallerstein R (1986). Forty-Two Lives in Treatment. Guilford Press, New York.
Wallerstein R (1995). The Talking Cures: The Psychoanalyses and the Psychotherapies. New Haven: Yale University Press.
Weinshel E (1984). Some Observations on the Psychoanalytic Process. Psychoanal. Q. 53:63-92.
Weinshel E (1990). Further Observations on The Psychoanalytic Process. Psychoanal. Q., 59:629-649.
APPENDIX
3 images are missing in this space
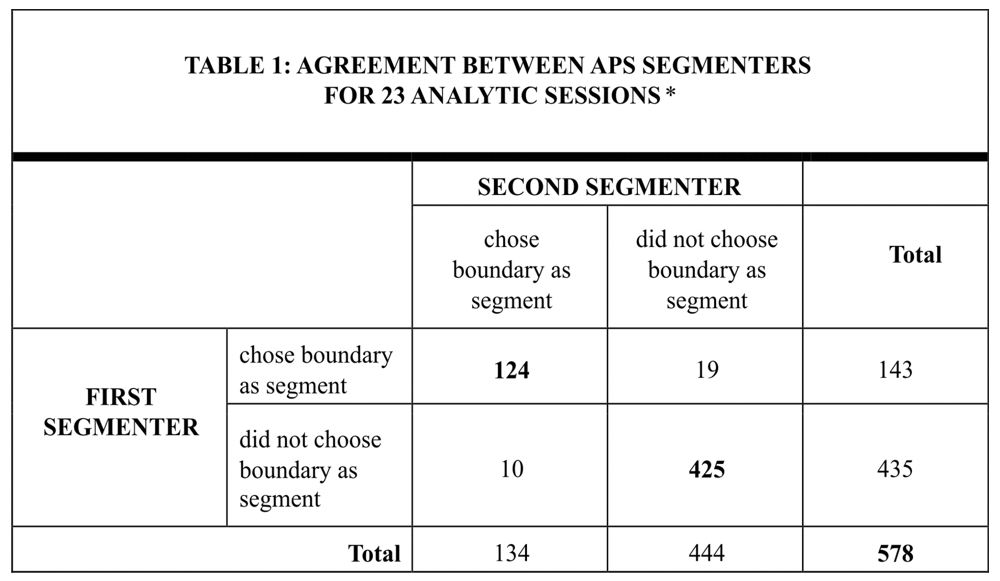
* Cohen Kappa = .86 Each segmenter marked those boundaries of turns of speech in the text where she felt there should be a division between segments. On rare occasions the raters would also divide a single turn of speech into more than one segment. For purposes of the count in Table 1, only turns of speech which could have been chosen as segment boundaries were counted, eliminating such turns of speech as “mmm-hmm” which were not eligible to be chose by definition, and eliminating those segments chosen during turns of speech. These eliminations were necessary in order to devise a fair test of the reliability of raters.
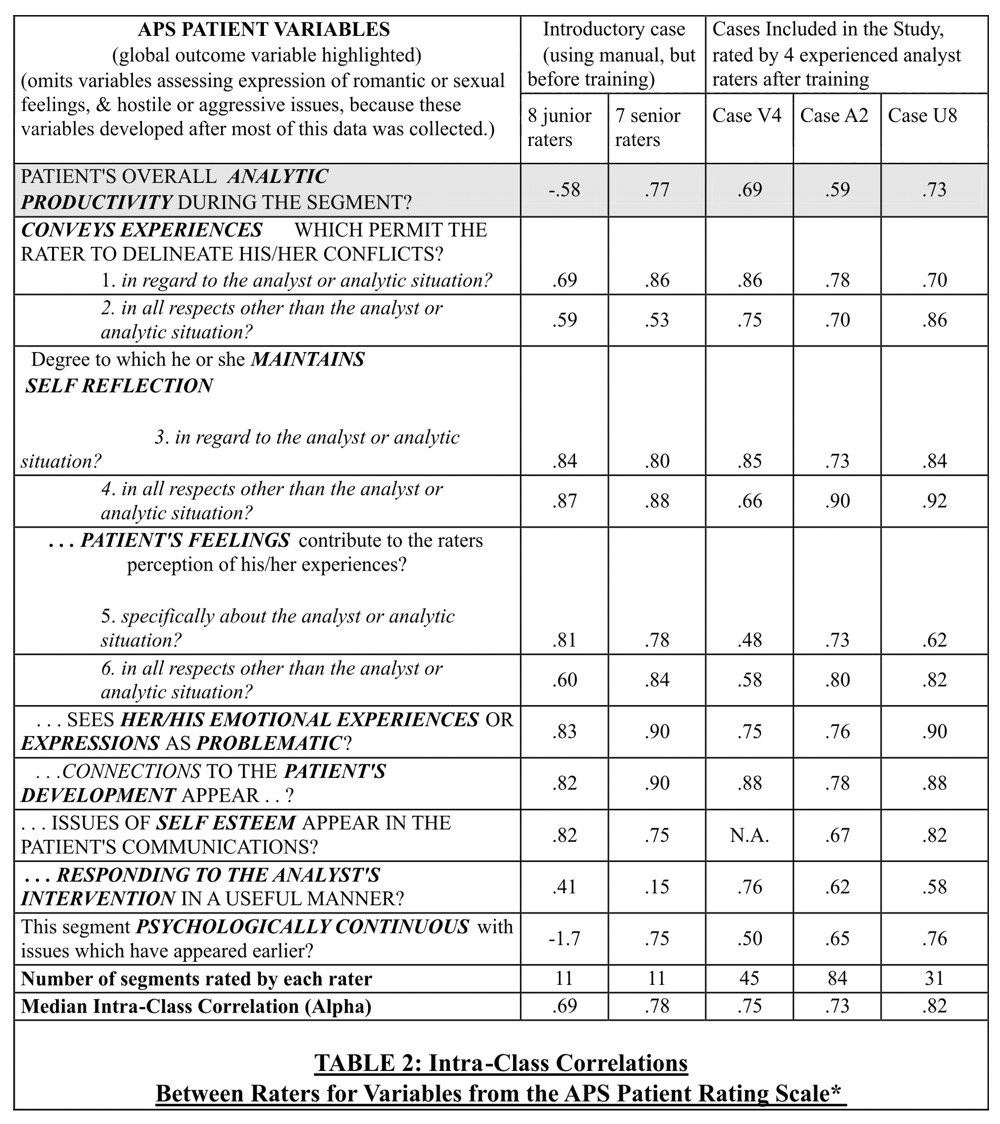
* Correlations can range from a minus number to zero for no reliability between raters, to a perfect reliability of 1.0. T1he APS Coding Manual was continually refined as raters moved from Case V4 to Case A2 to Case U8. This is reflected in improved reliabilities. Some variables had insufficient range for meaningful calculation of reliabilities for some cases. These are indicated by “N.A.” in the cells above. The intra-class correlation used is coefficient “alpha” from the SPSS reliability procedure, which is based upon the average between the four raters. This is an appropriate measure to report here since the results in our study are derived from scores averaging four raters. In this procedure, negative values should be regarded as equivalent to a zero correlation. Finally, The total patient segments are greater than the number included in the regression analysis because of merging of adjacent segments.
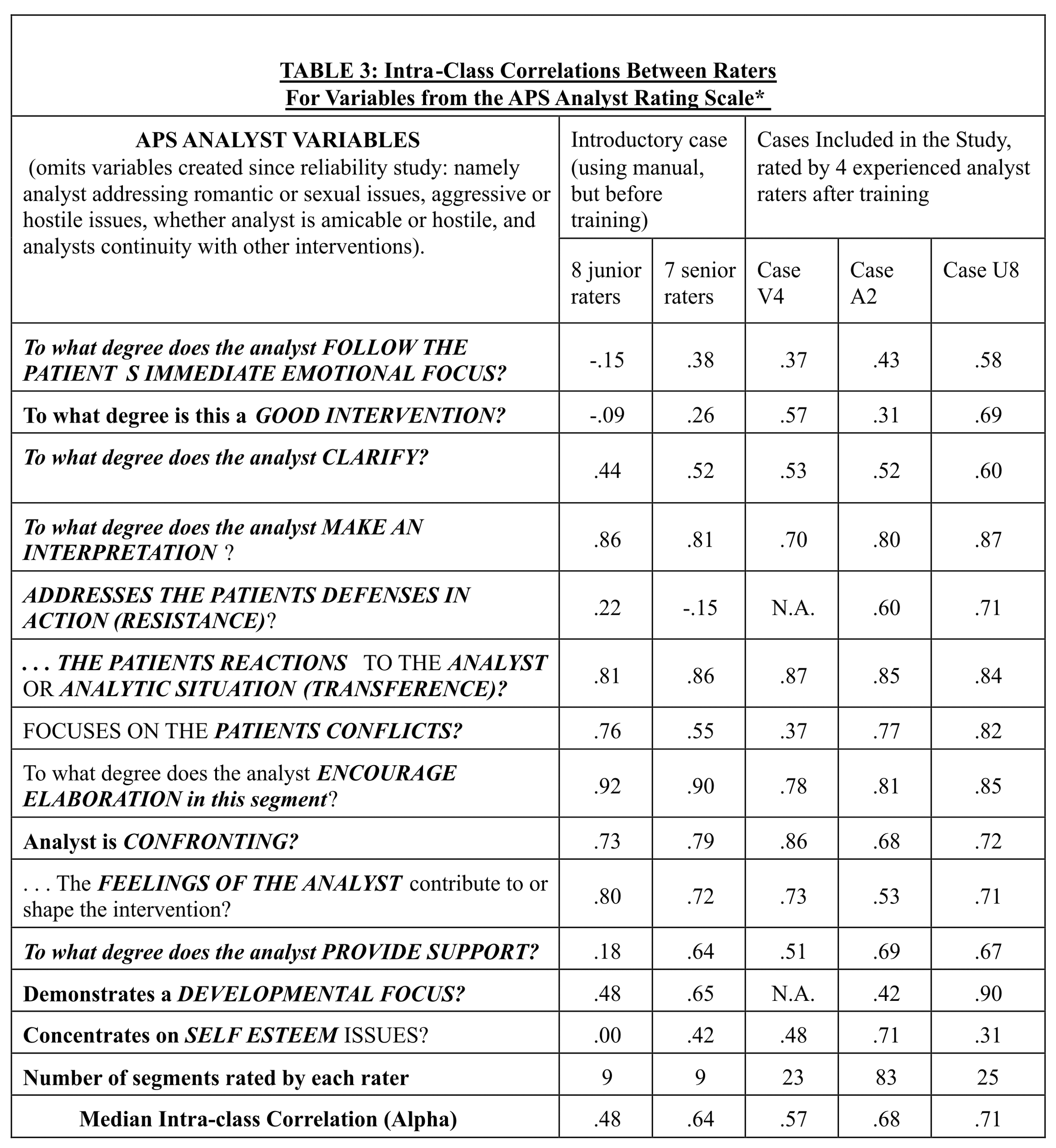
* Note for previous table also applies to this one. Of particular interest is the low agreement on good intervention for the patient A2. This reflected the analyst’s controversial technique, about which the raters had differing opinions. One rater’s mean score for goodness of intervention was twice that of another, and the differences between the four means was highly significant (F of 11.69 with 3 degrees of freedom). While there was evidently a high error variance for this patient-analyst pair, nevertheless the .31 value for alpha was significant at the .02 level.
END NOTES