Case Studies
Case Study: “Annie”
Annie is the case of a young housewife and mother who is afraid to venture outside her home. We provide actual transcripts of the first four meetings with her analyst, annotated by experienced psychoanalysts, along with audio versions (read by actors for confidentiality reasons). Each turn of speech (TOS) is numbered.
This very experienced analyst was able to engage his anxious patient, drawing her out to explore and come to an understanding of her issues. At the same time, the patient was committed to work hard at her treatment and was able to utilize what she learned from the sessions.
This case had a favorable outcome after two and a half years of treatment, starting at four times weekly, then twice weekly for the last year. In the first four sessions you can observe the way the patient utilizes the therapist’s communications, foreshadowing the favorable outcome.
We studied the outcome by evaluating her functioning early and late in her treatment. Details may be found at the end of this section under “Details of Annie’s changes during treatment”
You may prefer to read the case study below, in which we describe findings from the sessions, before studying the sessions themselves. Or, if you choose to go directly to the session transcripts or audio now, you will be invited to return here at the end of the sessions to review our findings.
If you start both the audio and the text of a given session, you can scroll along with the audio on your screen.
Session 1
Session 2
Session 3
Session 4
Annie Session #1: Most of this first session involves the therapist intervening with statements to encourage elaboration and provide support. Listening attentively after each question is in itself supportive. This is especially true for difficult subjects, such as why she needs help in the first place (this begins the session, #14), her sexual life (#70-94), her finances (#105), the nature of treatment (#114), and the possibility of ending her own life (#204).
Annie Session #2: The patient continues to explore her feelings about beginning treatment. The therapist remains supportive, but also increasingly explores her feelings evoked in this new relationship.
Annie Session #3: The therapist encourages the patient to reflect further on how she relates to him in the room, and he clarifies her anxieties and inhibitions in the unfolding relationship. The therapist remains near to the patient’s experience, while also providing salient, emotionally evocative responses to the patient’s uncomfortable feelings.
Annie Session #4: General: This session is rich in material, including a dream and towards the end, the revelation of an important experience of which the patient is ashamed. The session clearly illustrates the importance of both support and interpretation, in helping the patient understand the nature of her anxiety, as well as feel understood by the therapist.
Analysis of Therapist Communications
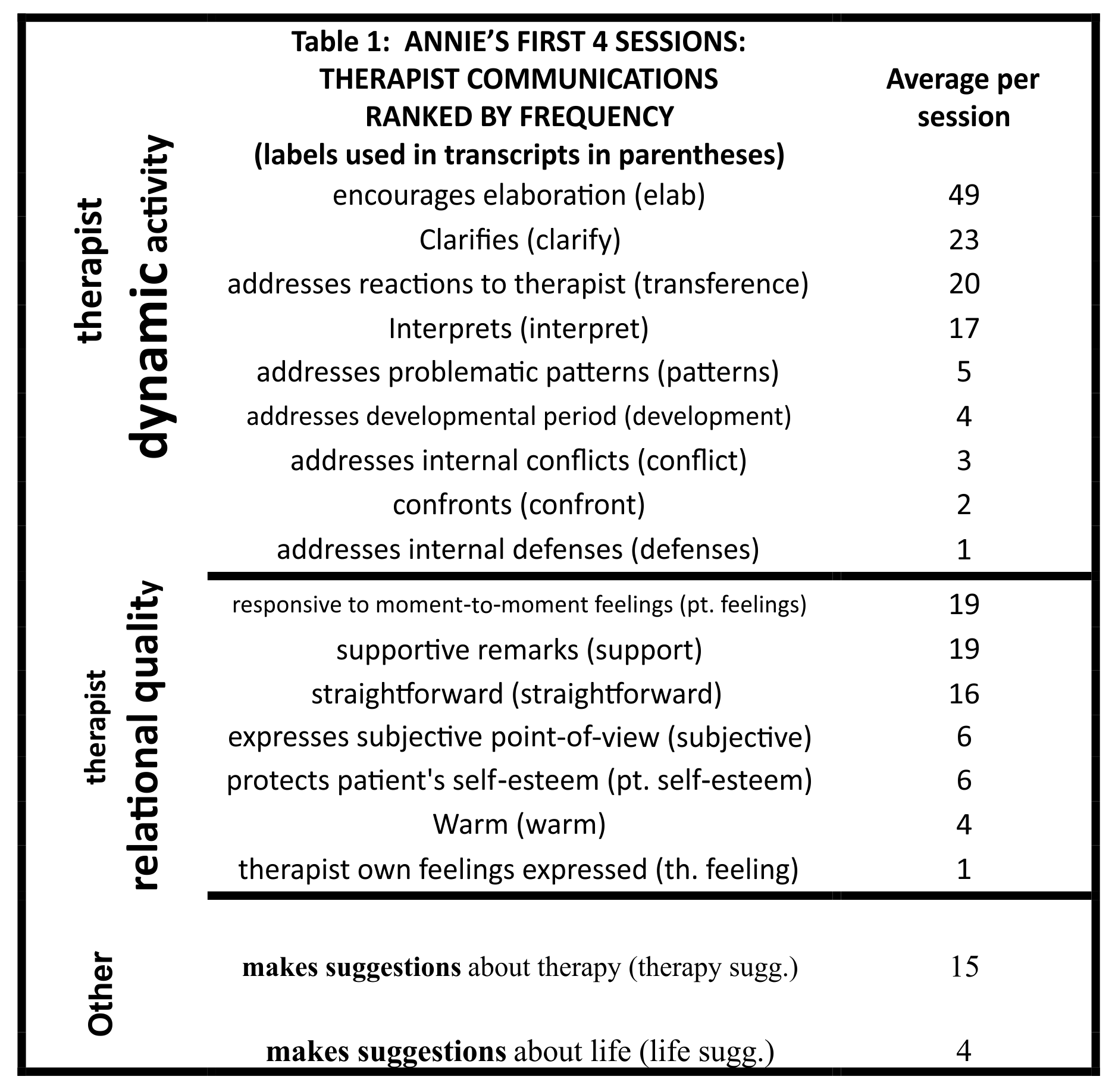
We made an intensive study of these first four sessions of Annie to develop a case-based example of what goes on between patient and therapist. Below is a table showing the nature of the communications by Annie’s therapist, from most to least prominent in each of three domains: therapist dynamic activity, therapist relational quality, and therapist suggestions. These categories are listed in Table 1, according to how frequently they occurred in these first four hours. Each therapist TOS could fit anywhere from none to multiple categories.
*For correlations among the categories, click here. For access to an excel file with Therapist’s Turns of Speech (TOS) scores for each session, click here.
Patterns of Communication
Our group of psychoanalytic psychotherapists has worked together for 35 years studying recordings of long-term treatments, to identify and describe what therapist and patient contribute to an evolving therapeutic experience (Waldron et al. 2004a, 2004b, 2013, 2018). We applied a factor analysis to therapist variables rated for 540 sessions from 27 psychoanalyses (Gazzillo et al. 2018).
Two factors emerged for therapists’ contributions: Therapist Dynamic Activity and Therapist Relational Quality, which are the primary source of the two headings in the charts. We supplemented this work by studying three instruments which were specifically developed to describe the full range of therapist actions in any psychotherapy. The third heading, Others, with the categories of suggestions about therapy and suggestions about life outside of therapy, was added based upon that study. Combining this work with other rating instruments, we developed the categories of communication used in this study. “We used the “Multi” as our starting point, and altered the categories to reflect a more specifically psychoanalytic focus (Kevin S. McCarthy & Jacques P. Barber (2009) The Multitheoretical List of Therapeutic Interventions (MULTI): Initial report, Psychotherapy Research, 19:1, 96-113, DOI: 10.1080/10503300802524343).” For details of this investigation click here.
These sessions are highly interactive. In contrast to the popular image of the therapist merely listening, there is a lot of back and forth between therapist and patient. The therapist had a total of 524 turns of speech (TOS).
Of TOS, 453 (86%) could be fitted into one or more of our categories (Table 1). The non-categorized TOS were generally ones in which the therapist participated in the conversation, such as “mm-hmm”, important to keep up his side of the conversation, but not fitting into any of the 18 categories. There is already a sense of forward movement in these four sessions, conveyed by the increasingly meaningful communication between the pair. The proportion of categorizable TOS rose from 81% in the first session to 92% in the fourth session.
Many of the therapist TOS fit into more than one category. Nearly half were rated as fitting two or more categories, and over 20% rated in three or four categories. There was substantial agreement between the raters (for reliability, click here.),
Here is an example from Annie’s fourth session, where the therapist’s remark in paragraph 23 was rated in three categories: as a clarification, as responsive to Annie’s moment-to-moment feelings, and as protecting her self-esteem. The surrounding conversation is included to give context.
. . .everything that came to my head, I was saying and, uh, when you start thinking about saying everything you’re thinking, it’s–you know, you wonder–gee….mmmmm.
21 T: Gee what?
22 P: You know, what does the person think of you, you know, that’s–I shouldn’t be worrying about that, you know.
23 T: You’re right. People very often, uh, don’t say certain things because if they think the other person will have a reaction that they don’t want them to have. But here, you are being asked to say everything so I guess the only way you can do that with any comfort at all would be if you had some conviction that I’m not using what you say to judge you or be critical or whatever.
24 P: Are you using it to (sighs) maybe, in the long run, uh….
25 T: To the best of my ability, I’ll use it to try to understand you.
The findings in Table 1 are striking. In terms of dynamic activity, the therapist is drawing out his patient in a very skilled manner, with a predominance of encouraging elaboration and clarifications, in this way shaping the dialog and their shared understanding of what she is suffering from. He is also very active addressing her feelings about the therapist and the therapeutic situation, which increases her sense of comfort and trust.
He does not hesitate to offer her his understanding as well, interpreting what she communicates, addressing problematic patterns, and connecting these to her developmental years. He occasionally addresses areas of her life where she is suffering from conflicting feelings, even using gentle confrontation to draw her attention to her conflicts.
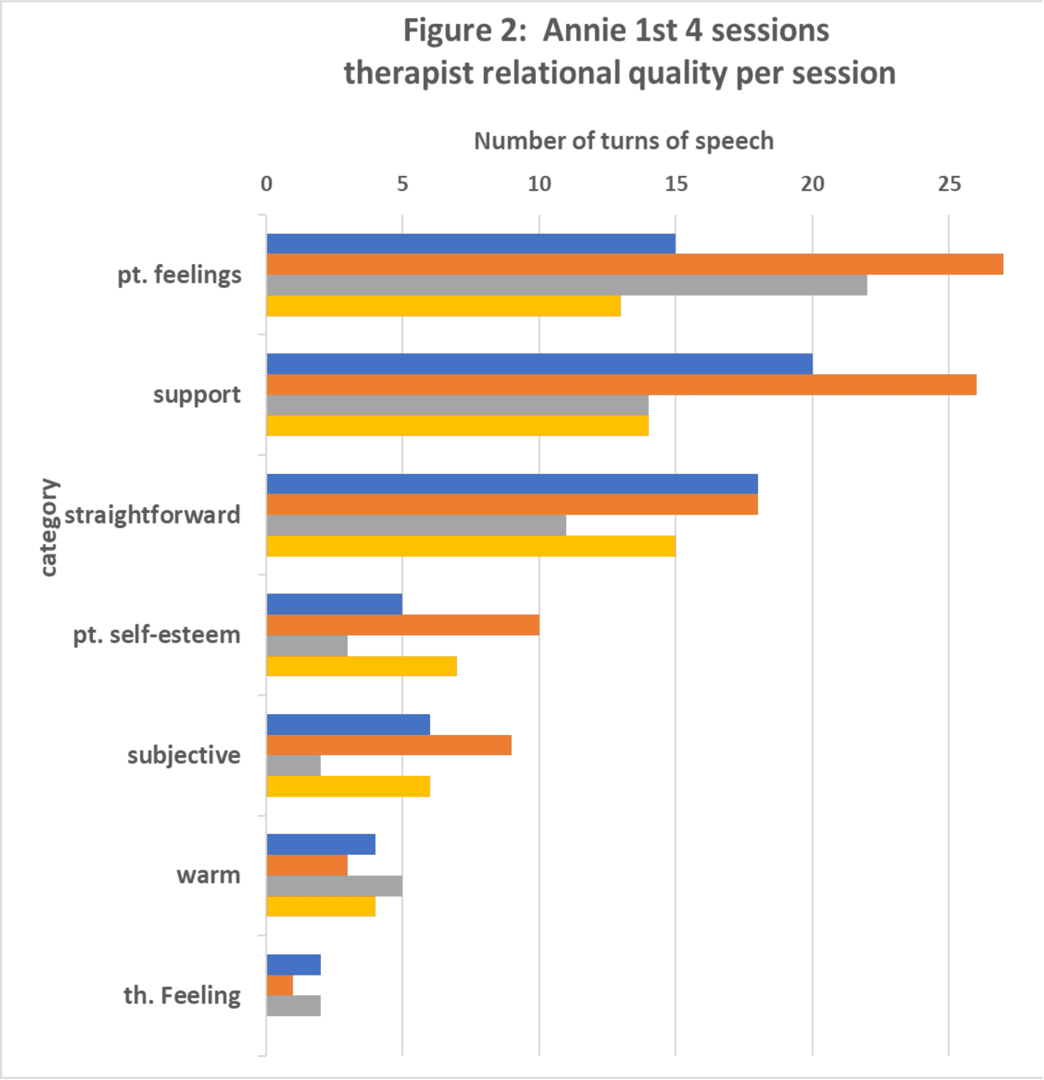
The experienced clinician-raters in our study group evaluated his relational quality, his tone and tactfulness quite positively: he is supportive, responsive to her moment-to-moment feelings, straightforward and willing to express his own point of view, warm, and careful to protect her self-esteem.
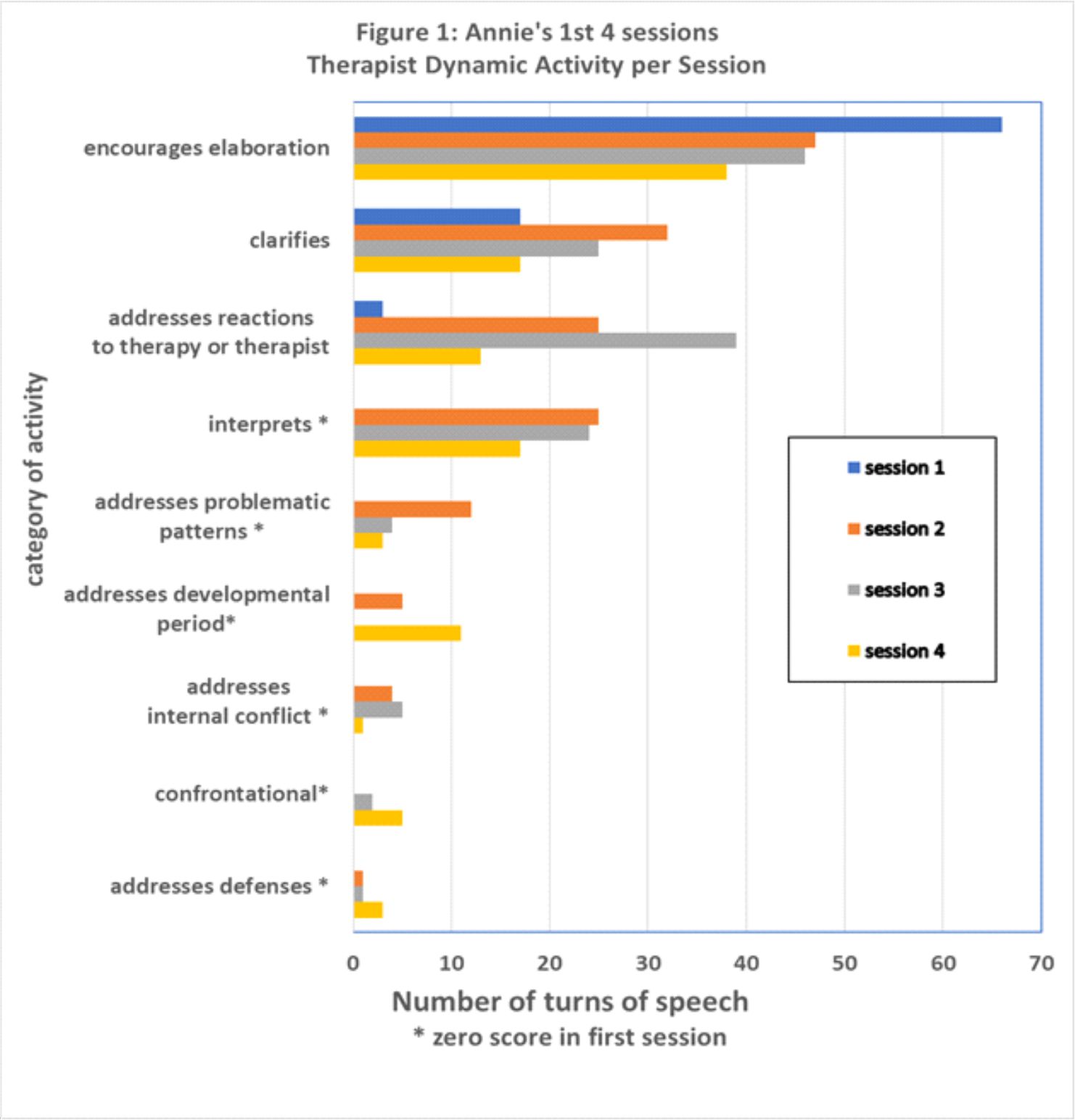
It is interesting to see how the type of communication changes over the course of the four sessions, shown in the charts below. In the first session, the therapist spends the most time encouraging elaboration and clarifying. He initially avoids interpreting, addressing maladaptive patterns, defenses or internal conflict, as the patient is quite anxious. Only as the patient becomes more comfortable does he approach her deeper issues.
Next Steps
If you have not done so already, we recommend taking the time now to familiarize yourself with this therapeutic pair by listening to and/or reading the first four sessions of the case of Annie. You will have a chance to see what the sessions were like, and your experience should enrich your study of the categories describing psychotherapy that we offer under the tab How Psychotherapy Works and in The PRC Manual.
Reliability of these classifications has been established over decades, using five-point Likert scales to characterize segments of sessions for their dynamic characteristics (Waldron et al. 2004a, b), or whole sessions for relational characteristics (Waldron et al. 2013). The average Spearman’s rho of the APS therapist variables was .94.
We checked the reliability of our two raters in the case of Annie (LR and SW). There were differences in the choice of particular TOS receiving relational ratings, such as when the therapist was rated as warm, or straightforward or addressing patient’s feelings, since this was an all-or-none rating, but the two analysts viewed the overall session in highly similar ways, as indicated in the following chart profiling their scores together.
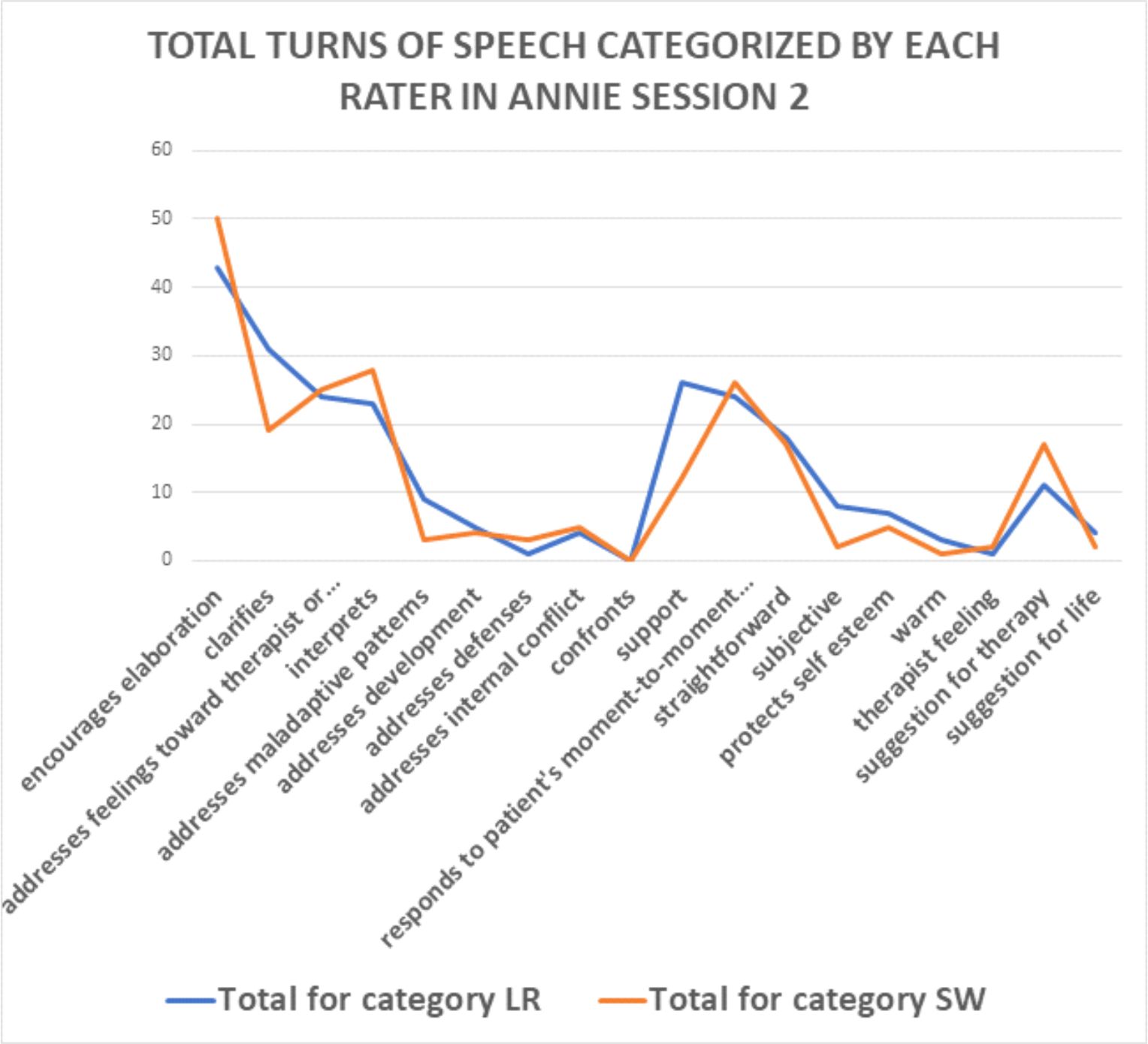
The final ratings used were by consensus.


Reliability of these classifications has been established over decades, using five-point Likert scales to characterize segments of sessions for their dynamic characteristics (Waldron et al. 2004a, b), or whole sessions for relational characteristics (Waldron et al. 2013). The average Spearman’s rho of the APS therapist variables was .94.
We checked the reliability of our two raters in the case of Annie (LR and SW). There were differences in the choice of particular TOS receiving relational ratings, such as when the therapist was rated as warm, or straightforward or addressing patient’s feelings, since this was an all-or-none rating, but the two analysts viewed the overall session in highly similar ways, as indicated in the following chart profiling their scores together.
The final ratings used were by consensus.