Psychodynamic Features CBT
Psychodynamic Features of Two Cognitive-Behavioural and One Psychodynamic Treatment Compared Using the Analytic Process Scales (APS)
Sherwood Waldron (New York) & Fonya Helm (Washington, DC)
For the APS Research Group ![]()
Summary
We examine the relationship between benefit in psychodynamic therapy, psychoanalysis and cognitive behaviour therapy (CBT), the techniques used by the therapist or analyst, and the quality of the work in a pilot study. We use a new instrument, the Analytic Process Scales (APS), along with a technique for segmenting sessions, to look at cause-and-effect sequences. Two CBT and one matched psychodynamic short-term therapy from the Montreal Pilot Study led by Perry and Robertson were studied. In all three therapies, psychodynamic techniques appeared substantially and were associated with immediate benefit. The judged quality of the interventions correlated strongly with immediate benefit. One CBT case is described, and findings from an early and late session illustrate the techniques used and the APS scores generated. This systematic and reliable approach to process analysis provides a method for clarifying differences and similarities in different therapies and modes of therapy.
In Press, Canadian Journal of Psychoanalysis, issue of December, 2004
There is an ongoing debate about what components of psychotherapy lead to benefit. Cognitive behavioural therapy (CBT) and psychodynamic therapies, including psychoanalysis, are often viewed by their proponents as constituting very different methods of working with individuals, and yet there is reason to doubt such allegations of different mechanisms of action (Frank, 1973). Recent studies (Leichsenring & Leibing, 2003; Svartberg, Stiles, & Seltzer, 2004) have shown nearly similar outcomes from the two techniques (with solid evidence of benefit to patients). The Svartberg et al. study is particularly notable because of the care with which each technique was carried out and evaluated, so that confidence may be placed in the quality of both treatments and their differentiation from each other. Yet the differences in technique between these two modalities do not so clearly correlate with differing outcomes (e.g., Gaston, Thompson, Gallagher, Cournoyer, & Gagnon, 1998).
Jones, Pulos, and Ablon (Jones & Pulos, 1993; Ablon & Jones, 1998) approached this issue by assessing psychodynamic elements in both CBT and dynamic treatments, correlating the degree of benefit with the degree that the treatments showed evidence of psychodynamic and CBT features. They found that the degree of benefit correlated with the presence of psychodynamic features in both groups, and not with the degree of presence of CBT features. Some of Svartberg et al.’s findings (2004) partially support this advantage in long-term benefit of psychodynamic technique, as do the findings of Grande et al. (2003). A residual problem has been the difficulty assessing both adherence and competence (Barber, Liese, & Abrams, 2003) or quality of intervention. The measurement of quality has particularly been problematic, so that most scales for the assessment of both types of therapy simply don’t evaluate quality or competence (e.g. Gaston et al. 1998; Trijsburg, Lietaer, Colijn, Abrahamse, Joosten, & Duivenvoorden, 2004). However, competence is assessed by the assessment instrument developed for cognitive analytic therapy (Bennett & Parrys, 2004), illustrating that the need for such measures is increasingly being met.
A group of psychoanalysts mostly from New York have developed a methodology for assessing psychodynamic (or psychoanalytic) features in treatments (Waldron et al. 2004a, 2004b). The instrument, the Analytic Process Scales or APS, is suitable for the study of psychodynamic features of any psychotherapy. Therefore, the APS research group decided to assess the psychodynamic features of some cognitive therapies collected and studied by the research group under the leadership of C. Perry and B. Robertson in Montreal (described in this issue (Trijsburg, Semeniuk & Perry 2004) The following report introduces the APS, and presents the results of applying the APS to two cognitive behavioral treatments and a matched psychodynamic treatment. Each treatment was limited to twenty sessions.
Developing a Set of Scales Assessing Psychodynamic Features
In 1985, a small group of psychotherapists in New York decided to study tape-recorded psychoanalyses, in order to study psychoanalytic work systematically, rather than to depend on reported clinical observations and individual case vignettes. Over the years, the group formulated variables that assess the psychoanalyst’s or psychotherapist=s work, the patient=s work, and the interaction between the two, using reliable ratings of central psychoanalytic dimensions.
Recorded sessions were divided into appropriate segments, each capturing a meaningful piece of the patient’s contribution, (a patient segment), and the therapist’s contribution, (a therapist segment). When there was a rapid interweaving of both contributions, a segment would be categorized as a joint segment. Then each segment was rated using the 14 patient variables, or the 18 therapist variables, or both. Each rating went from 0— – 1— – 2— – 3— – 4, i.e., a five-point Likert-type scale. An 80-page coding manual provided the definitions of each of our variables, with clinical illustrations at the zero level, the two level and the four level.
An initial study of nine sessions from three patients established that the variables can be rated reliably by experienced clinicians, using the APS Coding Manual.
In developing the variables, we used an inductive procedure, studying a series of recorded psychoanalyses together and gradually defining the characteristics of the treatment sessions studied. The raters would listen to and read the transcripts of at least two immediately prior sessions before making any ratings of subsequent sessions. The variables we developed were experience-near (at least for the clinicians), and descriptive of those features that we considered central to psychodynamic clinical work with patients. The coding manual is the centrepiece of our endeavours, capturing the essence of “core analytic activities” and describes them using case examples that have proved helpful in both studying and teaching psychoanalysis and dynamic psychotherapy.
Segmenting Sessions
We developed a procedure derived from the work of Stinson et al. (1994) to divide sessions into psychodynamically meaningful segments, each of which we rated on the relevant APS variables (that is, if the patient were talking, we would rate the patient variables, and if the therapist were talking we rated the therapist variables. If both patient and therapist were talking, we rated all the variables. We ended up with about 10 to 30 segments per session. The segmenting procedure is reliable (Waldron et al. 2004b), when carried out using our segmenting manual, anchored by case illustrations. The success of the segmenting procedure illustrates that psychoanalytically knowledgeable clinicians have a shared “feel” for natural dividing points in a session. The segmenting procedure allowed us to study what follows what, from which we can deduce what intervention is having an impact on the patient, and how is the patient’s material making it possible for the therapist to intervene. In other words to understand psychoanalytic process. The segmenting manual may be viewed along with other information about our work at our website, www.psychoanalyticresearch.org, and our coding manual may be obtained from the first author.
The APS Variables
As we appraise the degree to which psychoanalytic work is taking place in the psychotherapeutic situation, we want to know which participant is doing what kind of work. Most current authors consider a psychoanalytic or psychotherapeutic treatment to be the product of both parties, and emphasize the interaction between the two (for example, see Levine, 1994; Burland, 1997; Boesky, 1998). We therefore set ourselves the task of determining what is characteristically psychodynamic (psychoanalytic) about what the therapist contributes, what the patient contributes, and their interaction. By psychodynamic interaction we generally mean a mutual spiralling potentiation of understanding, with the therapist’s remarks leading to the development of further patient material and self reflection, and the patient’s remarks providing an opportunity for the therapist to add to further understanding in an evolving process (Schlesinger, 1974).
Five therapist variables assessing core analytic activities are the special focus of this paper:
clarification
interpretation
addressing defences
addressing transference, and
addressing inner conflicts
The raters estimate the degree to which each of these analytic activities is present, specifically disregarding the aptness or skill with which they are employed. Each of these elements is rated independently of the others, so that, for example, a given intervention could be rated “4”” for clarification, “2”” for interpretation, and “0”” for addressing transference.
Clarification is rated by the degree to which attention is called to insufficiently noticed surface features and how they are psychologically connected. Interpretation is rated according to how well the therapist’s intervention aims at transforming meaning by bringing aspects outside of awareness into full awareness. Addressing Defences refers to defenses active at this moment in the session, and assesses the degree of analytic focus on any measure the patient takes to avoid experiencing objectionable impulses, affects, thoughts, or fantasies. To be scored, addressing resistance must be manifest or, if inferred, easily identifiable by the rater and most therapists. Addressing transference is shorthand for pointing out the patient’s reactions to the therapist or to the therapeutic situation. Addressing inner conflicts is rated by the degree to which the therapist focuses on the patient’s conflicts in the segment—impulses or affects and their feared consequences or moral concerns.
The quality of therapeutic communication
The APS permits us to utilize clinician judgments of the quality of the therapist’s communication in each segment. This is important since studies have shown that clinicians vary their approach within any given therapeutic modality to meet the needs of patients, and this variation may in fact by the most important ingredient leading to therapeutic benefit. Our assessment of the quality of a communication rests on the aptness of the type of intervention, the usefulness of its content, and the skill with which the comment is made, including tact, timing, and language appeal.
Patient response to therapist communication: “patient productivity”
We are interested in therapist communications to patients because we presume that the nature and quality of these communications affects the patient for better or for worse. Our strategy for assessing benefit is to study the immediate impact upon the patient, and later to study the clinical course of the patient at termination and beyond. This latter step can not be accomplished except over a longer time period. However, a reasonable presumption is that therapeutic communication should show some cause-and-effect relation to patient response. Thus monitoring patient communications as sessions unfold should turn out to be an indicator of ultimate benefit. Furthermore, assessing the patients’ behaviors following therapist communication can reveal the interaction between patient and therapist, serving as a direct assessment of the impact of the therapeutic relationship. Of course, any such finding will need validation by follow-up studies as yet to be performed, showing whether observed quality of therapist communication and relation to subsequent patient communication is indeed prognostic of therapeutic benefit.
In order to accomplish this assessment, we evaluate what we call “patient productivity” in each patient segment. Our definition of patient productivity is described in our coding manual as follows:
Score a segment “”0”” when no apparent progress in understanding, nor in the involvement or collaboration in the analysis, nor in the nature of other developing emotional responses;
“ “2”” when there was moderate progress in the depth and breadth of understanding, or in emotional involvement and collaboration in the analysis, or in the nature of other emotional expressions;
“”4”” when the patient made strong progress.
Our patient productivity variable correlated most highly with all the other patient variables, (see website for list) hence appears to provide a valid general indicator of raters’ appraisal.
It is noteworthy that such a general clinical variable could be rated reliably, meaning that different analytic clinicians listening to several hours in a row to learn about the case, then rating a subsequent hour, gave scores for patient productivity which were very similar to one another, when they used our coding manual carefully, looking at the clinical descriptions for each level of productivity as well as the definitions, as they made their ratings.
Reliability of Various Raters Using the APS Coding Manual
The median alpha coefficient for our therapist variables was .71, and for the patient variables .82. Inexperienced and experienced clinicians were reliable after minimal training. But inexperienced clinicians benefited from more training in assessing the quality of interventions. In addition, most clinicians experience the study of the manual and of the clinical materials helpful to their clinical technique.
Core Analytic Activities, Quality of Communication, and Subsequent Patient Productivity
In our earlier study (Waldron et al. 2004a) we found in 117 segments from 9 analytic sessions with three different patient-analyst pairs, that average core analytic activity correlated .41 with patient productivity in the next segment, and the quality of the therapist communication correlated .61 with next patient productivity. These correlations represent strong effects, when there are so many other aspects to be taken into account in a complex therapeutic situation. A regression analysis showed that the single most important aspect was indeed the quality of the communication. These findings gave us reason to anticipate useful results from the present study.
Method of the Present Study
Cases were selected from a pilot study of combined antidepressant medications and 20 sessions of either CBT or dynamic psychotherapy for DSM-IV recurrent major depression made available by the Investigators, Drs. J. Christopher Perry, Elisabeth Banon, Serge Lecours, and Brian Robertson [see article in this issue by Trijsburg, Semeniuk and Perry]. All patients had moderately severe depression with an initial Hamilton Rating Scale for Depression of 17 or above. Three cases were selected: two CBT cases conducted by an experienced CBT therapist, and one dynamic case conducted by an experienced therapist who was also a fully trained psychoanalyst. The patients were treated on an approximately once weekly schedule for 20 sessions, and while the three patients differed in their initial levels of personality psychopathology, all patients showed marked improvement at the end of treatment. Ratings were carried out for one CBT case and the matched psychodynamic one by three psychology interns at the Karen Horney Clinic, under the joint guidance of Dr. Kenneth Winarick and Sherwood Waldron. The second CBT case was rated by three senior psychoanalysts, Fonya Helm, Robert Scharf and Sherwood Waldron, all part of the APS research group. Two early sessions were listened to, to provide context, then a subsequent session (usually the fifth session) was segmented and rated using the APS. Similarly, two late sessions were later listened to, and then a third late session (either the 18th or 19th) was rated using the APS. Mean scores were derived from the raters’ scores, and are the basis of the results.
Results
Table 1 shows our most important finding, but requires some introduction. Since APS scores for any APS variable in a segment can range from zero to four, and raters are asked to rate the presence of the various elements of treatment assessed by our variables, regardless of the ratings they have given on other variables, it is possible for raters to find substantial presence of none or all of the core analytic activity variables at once. For example, a therapist communication could be rated as addressing defense (3) as an interpretation (3), addressing aspects of the reaction of the patient to the analytic situation (2), and approaching the patient’s inner conflicts strongly (3). The same interpretive communication could have substantial elements of clarification as well (1.5). In order to convey our findings, we have elected to consider a rating of 1.5 or above (remember that the rating is the mean of 3 or 4 raters) as showing substantial presence of the variable. This level of the presence of core analytic activities is what is shown in Table 1.
[INSERT TABLE 1 ABOUT HERE]The two CBT cases showed substantial levels of most core analytic activities (evidence of the use of psychodynamic techniques) while the level of use in this sample was generally considerably less than that of the dynamic therapist. The degree to which the CBT therapist used clarification in both cases was one-half to two-thirds the level of the dynamic therapist, with approximately half of all therapist segments showing a substantial element of clarification. The level of interpreting was much lower than that for the dynamic therapist, averaging less than 10%, compared to nearly 40% for the segments of dynamic therapy. This level is still substantial. Approach to the patients’ defenses was low for all three cases, averaging only about 5%. The CBT therapist did not approach the patients’ reactions to the therapist at all in this sample, in contrast to a level of nearly 20% of the segments in the psychodynamic therapy. But the raters found the CBT therapist to be approaching the patients’ inner conflicts substantially (while the frequency of this approach by the psychodynamic therapist was still much higher, at the level of 50% of the segments). Overall, the mean core analytic activities levels for the two CBT cases were .61 and .68, whereas the dynamic case mean was 1.1, a highly significant difference by analysis of variance.
The next major finding is the relation between these core analytic activities and the patients’ subsequent productivity. For both of the CBT patients and for the patient treated psychodynamically, there was a substantial correlation between the average core analytic activity of a segment and the immediate next segment patient productivity, as may be seen in Table 2.
[INSERT TABLE 2 ABOUT HERE]Core analytic activities contributed moderately in each of the three cases to the patient’s immediate productivity in the next patient segment. A regression analysis showed that for each one-point change in core analytic activity, productivity increased by more than half a point. This degree of association is strong in a multivariate study of therapies. And the degree of association occurred both for the dynamic case, which we would expect based upon our previous work, and for the two CBT cases.
Our past study has shown that the quality of the therapist communication appears to be the most important element identified by the APS, in leading to increased patient productivity. Table 2 shows that indeed the quality of communication was important for all three of these cases, so that assessments of dynamic features and core analytic qualities both contribute importantly to our assessment of immediate patient benefit.
Core analytic activities include clarifying, interpreting, approaching defences manifest in the session, approaching reactions to the therapist, and approaching inner conflict. The two CBT patients show (Table 3) that the therapist approaching defences and inner conflicts correlates most highly with patient productivity, as has previously been found for dynamic patients. The scores for the dynamic patient are included for contrast. While there is some variability, the degree of consistency with previous findings and the levels found in such a small sample suggest the importance of the role of approaching patients’ conflicts and defences in both treatments. The very small number of segments qualifying in each of the three cases for addressing defences at least at a 1.5 level (five total in six sessions rated) does not provide an adequate test of the impact of these type of communications on patient productivity.
[INSERT TABLE 3 ABOUT HERE]A CBT Case Illustration
The following description of CBT case 09 is presented in detail to illustrate how the APS permits specific study of the psychodynamic features, and to illustrate the nature of the therapist communications which were scored, by 3 senior psychodynamic clinicians using the APS, as showing very substantial psychodynamic features. We believe it is worthwhile to present the summary to provide the “feel” of how this therapist worked with this patient. The summary was prepared by one of the senior raters based upon listening to three early and three late sessions, with no other source of information. The sessions rated on the APS were sessions 7 and 18 from a 20-session treatment. As mentioned before, each rater studied two sessions prior to the one being rated, for context.
The patient is a 29 year old married special education teacher, who became depressed after having a miscarriage, which disappointed her greatly. Her inner sense of self has been disrupted, and she feels that she is not normal. She experiences her symptoms as shameful. It is striking how often she laughs during the sessions in order to block a sad or angry feeling.
In Session 3, she shows a powerful tendency to deny and minimize her feelings. It is hard for her to join the therapist in thinking about her unhappiness. The therapist is sensitive and empathic as she questions her about the homework assignment of writing about her upsetting feelings and what triggered them. The therapist is especially good at staying close to the patient’s affect, clarifying the patient’s feelings and ideas, and communicating interest and involvement. Toward the end of the session, the patient is able to talk about her fear that she is being punished for a previous abortion and will not be able to carry a baby to term.
The therapist also is very good as sensing possible ruptures in the relationship and doing something about it. At one point in Session 5, the therapist realizes that she had used an example in a previous session about a cousin calling in the middle of the night to say she had delivered twins. The therapist expresses surprise at her insensitivity, and says she has been thinking about it the whole day after, saying, “how stupid of me! How could I give an example of a cousin delivering a baby, while you are dealing with miscarriage?” The patient says she didn’t even think about it, and the therapist again expresses surprise.
In Session 7, the first session rated, the therapist draws the patient out about her blocking and rejection of feelings of happiness about the pregnancy. The patient says that she doesn’t want to get excited about her new pregnancy in case something bad happens, and doesn’t want to take the chance of having to cope with other people’s feelings of sadness and unhappiness. As she is trying to explain, the therapist gets a little side-tracked, asking how her lack of feeling will protect others from their feelings, and the high point of the session is the patient’s expression of exasperation and anger, mixed with defensive laughter, at a person who said that she had had four miscarriages and two healthy children, implying that a miscarriage was not a big deal. The patient says, “God! Can people be so not helpful!”
After mentioning again that the patient doesn’t allow herself to feel positive emotions, the therapist shifts to questions about the patient’s day, sleeping and medication. Then the therapist presents some imagery relaxation exercises. The patient laughs a little during the imaginative presentations of scenes of a beach and a beautiful park, and says that she hasn’t been doing previously assigned exercises as much as she should. At the end of the session, the therapist focuses on the central issue of the patient’s need to learn more about how to regulate her affect by focusing on what triggers her emotional responses, and the patient responds by saying, “Excellent.”
By Sessions 14 and 16, the patient has passed the time of her previous miscarriage, is feeling much more secure about her pregnancy, and is feeling cautiously excited. The therapist emphasizes the forward movement, since earlier the patient did not allow herself to feel positive emotion. The patient acknowledges the helpfulness of the therapy overall and the relaxation exercises. Her material has become richer in terms of affect and the description of important friends/colleagues.
In Session 18, the second session rated, the therapist focuses on the underlying assumptions that lead to the patient’s automatic negative thoughts. The patient responds that from the time she was very young she was taught to do good, be perfect so that her parents wouldn’t be disappointed. The therapist points out that she didn’t want to be disappointed, either, and the patient agrees. They also talk about the patient’s ability to reorganize her work so that she isn’t so frustrated, and then they discuss her ideas about friendships. The patient describes how she had many guy friends and refused to date them, contrasting them with boyfriends. She then describes meeting her husband, and how her best friend predicted she would marry him when she herself had no idea that she would. When the therapist asks more, the patient explains that she had just ended a relationship with an abusive boyfriend and that her grandfather had recently died, so she and her husband got to know each other slowly. At first she did not feel attracted to him, but later on, she did. He was very different, very nice, and made her feel good about herself. The therapist clarifies that she was very flexible, as opposed to imposing categories on the relationship, and that it had worked out well for her.
The patient also discusses how she is very close to her parents, calling them every day or two, but doesn’t want them to know that she is in therapy. She says she took a long time to tell her husband, and she doesn’t want anyone to know. Her shame at her loss of control of her emotions is very great, and the therapist is sensitive and empathic as she discusses the shame about seeking treatment from the point of view of understanding core beliefs. The patient opens up about her lonely childhood and how she was self-sufficient very early, playing alone and coming home from elementary school to fix her lunch, eat it by herself and wash the dishes. They then discuss when it is appropriate to seek the help of others. The session ends with a discussion of different categories of friends, with the therapist pointing out that the patient has been believing there was only one category.
Application of the APS to Session 7 of This Treatment
In order to explore the session in detail, the following graphs will present the core analytic activities, the quality of the communication in each segment, and how productive the patient was judged to be after the segment, along with our comments about what is going on between patient and therapist.
The vertical axis shows the APS score, which can range from zero to 4, with one line showing how good the intervention was judged to be, and the other showing the patient productivity in the next segment.
Note that the patient productivity is a lag variable: for purposes of display, the patient productivity which followed the therapist communication is shown at the same place on these graphs. For example, at segment 14, the analyst’s intervention was rated “2,””, and the patient productivity jumped up to “2” as well. But this is actually the productivity of segment 15. It is charted this way because it is easier to see what relates to what.
We have explained that we have five core analytic activities. However, in this sample the therapist never addressed the patient’s transference manifestations, and therefore this core analytic activity is not charted. The remaining four core analytic activities are shown as areas on this chart, which are added to each other, so that the peaks of core analytic activity of whatever kind may be seen by the general profile of the areas shown, and at the same time the vertical dimension of each area at each segment may be inspected to see what were the specific core analytic activities present (e.g., segment 14 interpretation = 3–-2.3 or 0.7 points on the APS scale from 1 to 4).
Figure 1 shows the specified APS scores from session 7, and the second figure shows session 18, toward the end of this 20-session treatment.
Below we examine several of the peaks of these two sessions, describing the actual interventions and the patient’s responses. The arrows draw attention to the specific segment being described.
The first part of session 7 (figure 2) shows the close interweaving of the cognitive approach with a careful approach to the patient’s affects and defences..
The therapist first makes a defense interpretation of the patient’s repression of her affect: “You’re not allowing yourself to feel?” The therapist’s intervention also addresses conflict between the defense of repression and the drive derivative that accompany the repressed the affect: “[I]f we start from thinking, maybe we will see if you feel anything.” This intervention is also a good intervention, because the patient’s productivity increases: the patient says she is too scared to feel anything and that it is a “mechanism of protection” (a defence).).
Segments 10 & 11 continued the elaboration of the patient’s avoidance of feelings of excitement, happiness and anticipation, and how much of the time she is suffering from feelings of fear, and even wonders if she is imagining blood on the tissue when she wipes herself, and asks her husband to come and look.
Segments 12 and 13 follow from T asking her about her appointment with the new doctor next week, and she makes clear her feelings of anticipatory helplessness and powerlessness.
The next image (figure 3) illustrates how the sensitive approach of the therapist is followed by a much more direct expression of her fear that somehow she might contribute to the painful loss.
]
The therapist addresses conflict: “How are you feeling about the pregnancy?” The patient laughs inappropriately, indicating anxiety since she expects the therapist to say again that she is not feeling appropriately happy. The patient is continuing to process her own self-criticism and the implicit criticism of the therapist’s previous defense interpretation. (Defence interpretations always give the patient the impression that the therapist is saying she is doing it wrong (Goldberger, 1995)). The patient’s inappropriate laughter blocks a more appropriate expression of anger and indicates an intensification of the conflict. The laughter is also a lower level of defense that also defends against the drive derivatives attached to the repressed anger. The patient says she should be happy about the pregnancy, expressing again both her own self-criticism and a fear that the therapist will stir up more anger. Instead, the therapist interprets another defence, the reaction formation against the anger at the therapist. The therapist says that the patient is apologizing for not feeling, and then goes for a supportive intervention, saying that whatever the patient is feeling is her feeling. The supportive intervention alleviates the patient’s anxiety and unconscious anger and strengthens the alliance in the short term. The patient is then able to elaborate about her fear that if she is not happy, the baby will leave. Again, the patient’s productivity is very great. She is working with the uncanny idea of a baby that has intentionality and can feel anger at the mother’s thoughts and retaliate by deciding to be born too early. After the alliance is further strengthened by the therapist’s empathic listening, the therapist is then able go back to another interpretation of the defense of repression, saying the patient is afraid to be happy and is “keeping [her feeling of happiness] on, on check.”
Application of the APS to Session 18
We first present in figure 4 the graphing of the core analytic activities, good intervention and patient productivity for the entire session.
[INSERT FIGURES 4& 5 ABOUT HERE]In Session 18, Segments 31–-35, the therapist does more clarification and supportive interventions. In segment 31, she compliments the patient on coming to therapy, saying they need to work on her shame and how to recognize when it is appropriate to ask people for help. Both working on shame and recognizing when to ask for help are “leading edge: interpretations (Miller, 1985). According to the APS, they are judged to be good interpretations and they lead to greater patient productivity. The patient has much greater access to her feelings of loneliness and produces new historical information. She says, “My parents never put us in group sports. . . . ….I ended up growing up very alone. Playing with my own little Barbies. . . . ….I was in elementary school, coming home, eating lunch by myself, making my own lunch . . . …[and]washing my dishes.”
[INSERT FIGURE 6 ABOUT HERE]In Segment 33 (figure 6), the therapist, according the APS criteria, addresses conflict, and makes a combination of a clarification and interpretation when she says there are circumstances in which the patient needs to be more flexible and depend on other people so she can respond to a crisis situation. The therapist’s intervention is also supportive in that it is empathic and gives the patient permission to have normal dependency needs. Moreover, the intervention addresses the patient’s goal of becoming more skillfully assertive in responding to a crisis situation, a “leading edge” interpretation, according to self psychological principles. According to the APS, the therapist’s work here is also judged to be a good intervention, and leads to greater patient productivity, as the patient agrees to challenge her idea of being self-sufficient.
[INSERT FIGURE 7 ABOUT HERE]In Segment 35 and response (figure 7), the therapist addresses conflict and clarifies by saying that the patient has a core belief that it is good to be independent. But she will not always be able to be self sufficient. When she has a baby, and if she moves to another city, she will need a lot of things from others. These statements are judged to be a good intervention and the patient says she’ll need her husband for sure, and then admitted there could be many other things where she will need help.
Discussion
We see that it is only in the late session that the patient began to address comments to her feelings about the therapist. This change would imply to us that the therapist’s sensitive repeated approaches to the patient’s conflicts enabled her to alter her characteristic, rigid and unforgiving ways of handling her dependency needs and longings. We also had the impression that the CBT format for the session enabled the patient to relate well to the therapy in a way that might not have been so likely had she been in a more unstructured setting customary in a psychodynamic treatment. Both the greater structure in the session and the greater activity level of the therapist provide more support and are less disruptive to the patient’s inner sense of balance and level of comfort than the therapist’s relative silence that occurs in most psychodynamic psychotherapy and psychoanalysis. Furthermore, the patient characteristically needed to ward off painful affects and therefore was much more comfortable with a format emphasizing what she should do about her symptoms, rather than one whose manifest focus was on what she was feeling and thinking.
The APS provides an opportunity to approach systematically what is taking place in a given treatment, whatever it is called, and to evaluate how therapist comments show evidence of facilitating the patient’s participation (productivity) or not.
This study is of course preliminary and presented as a demonstration project. The sample is small. The raters are all psychodynamic clinicians, and it is clearly necessary to compare APS ratings of both CBT and psychodynamic cases given by CBT clinicians, and to compare ratings by both groups of clinicians on other scales reflecting CBT-oriented techniques, as is illustrated in the article by Trijsburg et al. in this issue. We hope that such collaboration will take place soon. Furthermore, there is the possibility of theoretical bias affecting the ratings, since the same individuals rated the analyst communications and the patient responses. In our earlier study (Waldron et al. 2004a) we developed substantial evidence that bias does not account for the APS findings. Nevertheless, our conclusions would rest on a firmer foundation if it turns out that clinicians trained in CBT, psychodynamic therapy and psychoanalysis turned out to judge the therapist communications rather similarly.
Variables could also be added to the APS to assess CBT aspects of treatments specifically. We are currently establishing a working group in order to accomplish this goal, first by studying the various rating instruments already in existence (Bennett & Parrys, 2004; Trijsburg et al., 2004; Gaston et al., 1998) and using them or adapting their scales. We need to add CBT examples to our coding manual, because our senior clinician raters had difficulties assessing some of the CBT interventions on a number of dimensions, such as clarifying, interpreting, providing support, and the quality of the intervention, since the coding manual was developed originally using only psychodynamic sessions as examples. Convergent and discriminant validity, in comparison to the other CBT scales mentioned above, need to be investigated. The particular advantage of using the APS is that cause-and-effect relationships between therapeutic technique and immediate patient productivity and benefit can be investigated using dimensions that make clinical sense, and that have been at the centre of many conceptualizations of psychotherapy. In studying CBT, the APS could help to delineate the way that CBT interventions approaching conflict and defence are conceptually related to psychodynamic interventions.
Finally, further research may show that psychodynamic therapies utilize CBT techniques (without attribution), in a way parallel to the discovery that there are important psychodynamic elements in the CBT treatments studied.
References
Ablon J., &, Jones E. E. (1998). How expert clinicians’ prototypes of an ideal treatment correlate with outcome in psychodynamic and cognitive-behavioral therapy. Psychotherapy Research,Psychother Res 8, 71–83.
Barber, J. P., Liese, B. S., & Abrams, M. J. (2003). Development of the cognitive therapy adherence and competence scale. Psychotherapy Research, 13, 205–-221.
Bennett, D., & Parrys, G. (2004). A measure of psychotherapeutic competence derived from cognitive analytic therapy. Psychotherapy Research, 14, 176–-192.
Boesky, D. (1998). Clinical Evidence and Multiple Models: New Responsibilities. J. Amer. Psychoanal. Assn., 46:1013-1020
Burland, J. A. (1997). The Role Of Working Through In Bringing About Psychoanalytic Change. Int. J. Psycho-Anal., 78:469-484
Frank, J. (1973). Persuasion and healing. Baltimore: Johns Hopkins University Press.
Gaston, L., Thompson, L., Gallagher, D., Cournoyer, L. G., & Gagnon, R. (1998). Alliance, technique, and their interactions in predicting outcome of behavioral, cognitive, and brief dynamic therapy. Psychotherapy Research, 8, 190–-209.
Goldberger, M. (1995). The couch as defenseDefense and as potential for enactment. PsychoanalyticEnactment. Psychoanal Quarterly, 64, 23–-42.
Grande, T., Rudolf, G., Oberbracht, C., & Pauli-Magnus, C. (2003). Progressive changes in patients’ lives after psychotherapy: Which treatment effects support them? Psychotherapy Research, 13, 43–-58.
Jones, E. E. and Pulos, S. M..(1993). Comparing the process in psychodynamic and cognitive-behavioral therapies. J. Consult. & Clin. Psychol., 61(2): 306-316.
Leichsenring, F., & Leibing, E. (2003). The effectiveness of psychodynamic therapy and cognitive behavior therapy in the treatment of personality disorders: A meta-analysis. American Journal of Psychiatry, 160, 1223–-1232.
Levine, H. B. (1994). The Analyst’s Participation in the Analytic Process. Int. J. Psycho-Anal., 75:665-676
Miller, J. P. (1985). How Kohut actually worked. In Arnold Goldberg (Ed.), Progress in Self Psychology (Vol. 1) (pp. 13–30). New York: Guilford Press-.
Stinson C., Milbrath C., Reidbord S., &, Bucci, W. (1994). Thematic segmentation of psychotherapy transcripts for convergent analyses. Psychotherapy, 31, 36–48.
Svartberg, M., Stiles, T., & Seltzer, M. (2004). Randomized, controlled trial of the effectiveness of short-term dynamic psychotherapy and cognitive therapy for Cluster C personality disorders. American Journal of Psychiatry, 161, 810–-817.
Trijsburg, R. W., Lietaer, G., Colijn, S., Abrahamse, R. M., Joosten, S., & Duivenvoorden, H. J. (2004). Construct validity of the Comprehensive Psychotherapeutic Interventions Rating Scale. Psychotherapy Research, 14, 346–-366.
Trijsburg, R.W., Semeniuk, T. & Perry, J.C. (2004). An empirical study of the differences in techniques between dynamic psychotherapy and cognitive behavioural therapy for recurrent major depression. This Issue.
Waldron, S., Scharf, R. D., Crouse, J., Firestein, S. K.,. Burton, A., & Hurst, D. (2004). Saying the right thing at the right time: A view through the lens of the Analytic Process Scales (APS). Psychoanalytic Quarterly, 73: 1079-1125…
Waldron, S., Scharf, R. D., Hurst, D., Firestein, S. K., & Burton, A. (2004). What happens in a psychoanalysis: A view through the lens of the Analytic Process Scales (APS). International Journal of Psychoanalysis, 85, 443–-466.
e-mail of first author: woodywald@earthlink.net
(image goes here)
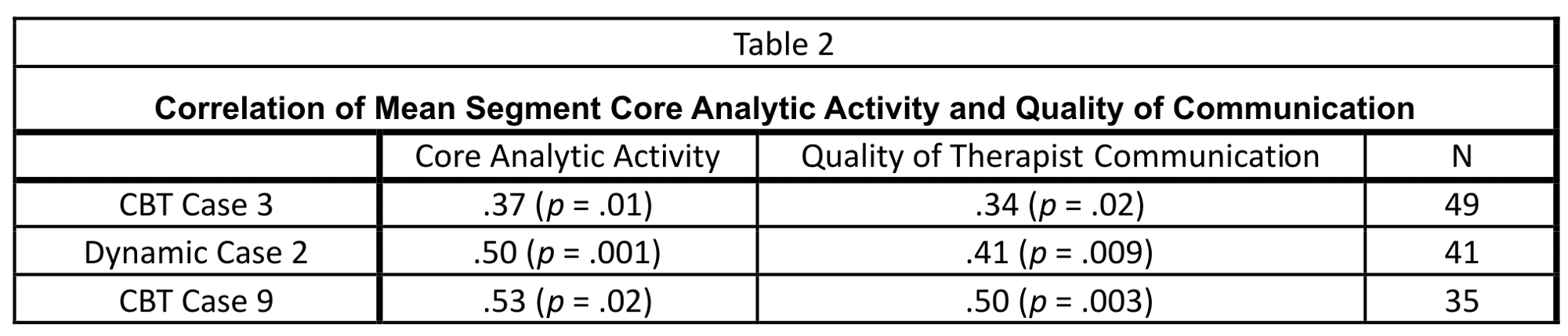

FIGURE 1: PATIENT 9 SESSION 7
FIGURE 2: PATIENT 9 SESSION 7, FIRST PART
FIGURE 3: PATIENT 9 SESSION 7, SEGMENTS 14 & 15 & RESPONSE
FIGURE 4: PATIENT 9 SESSION 18 ALL SEGMENTS
FIGURE 5: PATIENT 9 SESSION 18 SEGMENT 31 & RESPONSE
FIGURE 6: PATIENT 9 SESSION 18 SEGMENT 33 & RESPONSE
FIGURE 7: PATIENT 9 SESSION 18 SEGMENT 35 & RESPONSE[/vc_column_text][/vc_column][/vc_row]