Saying the Right Thing at the Right Time:
A View through the Lens of the Analytic Process Scales (APS)
© 2004, Sherwood Waldron, Robert Scharf, James Crouse, Stephen Firestein, Anna Burton, & David Hurst.
Published in The Psychoanalytic Quarterly,73: 1079-1125.
Authors
Sherwood Waldron, M.D.
1235 Park Avenue, Suite 1B
New York, NY 10128
(212) 722-2248
Robert D. Scharf, M.D.
207 East 74<sup>th</sup> Street
New York, NY 10021
(212) 988-4145
James Crouse, Ph.D.
575 Main Street, #1207
New York, NY 10044
(212) 572-9973
Stephen K. Firestein, M.D.
8 East 96<sup>th</sup> Street
New York, NY 10128
(212) 831-4554
Anna Burton, M.D.
163 Engle Street, Bldg. 2
Englewood, NJ 07631
(201) 567-4633
David Hurst, M.D.
601 Emerson Street
Denver, CO 80218
(303) 832-5024
ABSTRACT
Skillful psychoanalytic technique presumably involves knowing what to say, and when and how to say it. Does skillful technique have a positive impact upon the patient? This study used ratings by experienced analysts using the Analytic Process Scales (APS), a research instrument for assessing recorded psychoanalyses, to examine analytic interventions and patient productivity (greater understanding, affective engagement in the analytic process, etc.). In three analytic cases, we found significant correlations between core analytic activities (e.g., interpreting defenses, transference and conflicts) and patient productivity immediately following the intervention, but only if carried out skillfully. Findings were independently replicated by psychology interns.
How to measure psychoanalytic processes remains a problem more than a hundred years after the invention of the procedure of psychoanalysis. Many psychoanalysts continue to question the value of systematic empirical research in our discipline. They believe that measuring and assessing their work would not only be intrusive and distorting, but would ultimately fail to capture the uniqueness of analytic interventions, which are often tailored to subtle changes in patient, analyst, and the relationship between them. They also fear that research might understate the effectiveness of analytic therapy. In addition, most analysts object to tape-recording their work for research purposes, in part because they feel it would violate their relationship with the patient. However, the lack of sufficient systematic study of this therapeutic procedure has reduced its acceptability to a broader scientific audience, and has reduced the possibility of comparing it systematically to other treatments, in turn contributing to a reduction of public support. It may also have slowed its internal development, since the accumulation of systematic knowledge may lead to discoveries improving the efficacy of psychoanalytic treatments..
Summary of the Literature
The problem of how to measure the relationship between treatment process and benefit is shared by the fields of psychoanalysis and psychotherapy. There have been a number of prior studies of the immediate effects of interventions on the patient or the process, such as that of Garduk and Haggard (1972), Malan (1976), O’Malley, Suh and Strupp (1983), Luborsky et al. (1989) and Gedo and Schaffer (1989). However, the quality of interventions has generally not been assessed in studying immediate or long-term effects, in part because methods for such assessment have not been sufficiently developed. In this paper we use the term “quality” to refer to clinician judgments of the way the comments of the analyst or therapist may be expected to affect the patient, including the aptness of the intervention’s type, the potential usefulness of its content, and the skill and tactfulness of its presentation (see appendix 2). In a review published by NIMH, Borkovec and Miranda (1996) pointed out: “Despite initial attempts for some types of therapy, there is no valid way to measure quality for any therapy technique.”
However, there are several promising lines of research related to the quality of analytic technique. Jones and co-workers (Jones and Windholz 1990, Jones and Pulos, 1993, Ablon and Jones 1998) have reliably characterized the nature of the therapist’s approach to the patient. They make a clear distinction between psychodynamic and cognitive-behavioral features, demonstrating that the former correlate with successful outcomes while the latter do not, both in a sample of patients treated by psychodynamic therapy and another treated by cognitive-behavioral therapy. This finding was based upon measuring the techniques used by the therapists without attempting to measure their quality. “Quality” was measured in an interesting small study by Glass et al. (1989), demonstrating a substantial relationship between skillful dynamic exploration and outcome in schizophrenia.
The studies carried out by Joseph Weiss, Harold Sampson and co-workers have importantly contributed to assessing the quality of interventions (Weiss & Sampson 1986). In their view, interventions need to conform to the patient’s plan for therapy, that is, the patient knows at some level what help is needed, and tests (purposefully, though not consciously) the therapist’s ability to provide it. If the therapist intervenes in a way that is “pro-plan,” the patient improves (Norville et al. 1996). This group of researchers has been very careful in supporting their claims with evidence, which was primarily derived from audiotaped psychoanalyses and psychotherapies.
Two other sets of investigations provide more indirect approaches to quality. Dahl and co-workers (1988, 1991) have shown a relationship between interventions that address patterns of repetitive maladaptive emotion structures (which they call FRAMES) and the substantial reduction of those patterns, so that the quality of interventions can be assessed by how accurately they address the patient’s FRAMES. Similarly, Luborsky and co-workers (1988,1998) have demonstrated a relationship between addressing Core Conflictual Relationship Themes (CCRT) and benefit.
Caston et al.’s (1986) study of the effect of interpretiveness on the patient’s insight and boldness has assessed central psychoanalytic concepts with high reliability. It showed a significant impact, comparable to findings we report here, which we will refer to further in the discussion.
We believe that our group has taken an important step by developing an instrument, the Analytic Process Scales (APS), which makes it possible to study the impact of the quality of analysts’ interventions on patients’ immediately subsequent analytic productivity.
We have previously described (Waldron et al. 2003) our working conceptualizations of the psychoanalytic process, as they evolved in the course of developing the APS and coding manual, and found expression as APS variables. A distillation of these ideas defines the psychoanalytic process as a special interactive dialogue between patient and analyst, aimed at lessening the patient’s emotional conflicts, suffering, and dysfunctions. If the procedure is successful, the patient communicates increasingly unconstrained and affectively expressive associations and reflections (which we consider to be a productive response by the patient to the analyst’s communication). The analyst contributes to the conversation from time to time with requests for elaboration, clarifications, interpretations, or support, aimed at facilitating the patient’s communications and transforming the patient’s awareness. Mindful of the patient’s self-esteem and immediate emotional focus, interventions approach conflict, transference, and resistance. With the unfolding interaction between the patient and analyst, connections between the present, past, and analytic situation emerge. These aspects are illustrated in Appendix 2, which presents two variables from the APS Coding Manual used to assess the quality of an intervention, and the productivity of a patient’s communication.
METHOD
Development of the Analytic Process Scales (APS)
A review of the APS and its development will permit the reader to understand our findings and assess the validity of our claims. ![]() Our group of mostly New York-based experienced psychoanalysts has spent the past eighteen years devising the means to assess tape-recorded psychoanalyses in a way which reflects clinical psychoanalytic features as closely as possible, while inevitably limited by the perspectives we each bring to psychoanalytic work. Our research group is led by Sherwood Waldron Jr., and includes as directors Anna Burton, James Crouse, Shuki Cohen, Stephen Firestein, Fonya Helm, David Hurst, John Lundin, Seymour Moscovitz, Robert Scharf and Kenneth Winarick,.
Our group of mostly New York-based experienced psychoanalysts has spent the past eighteen years devising the means to assess tape-recorded psychoanalyses in a way which reflects clinical psychoanalytic features as closely as possible, while inevitably limited by the perspectives we each bring to psychoanalytic work. Our research group is led by Sherwood Waldron Jr., and includes as directors Anna Burton, James Crouse, Shuki Cohen, Stephen Firestein, Fonya Helm, David Hurst, John Lundin, Seymour Moscovitz, Robert Scharf and Kenneth Winarick,. ![]() Five of us are full-time practitioners, each with more than thirty-five years of clinical experience and Dr. Crouse is an experienced social scientist who has played a central role in evaluating our data. Our other directors are younger members with a special interest in research. We aimed at studying the nature of analytic interventions, the nature of the patient’s contributions, and the relationships and interactions between them. We tried to use methods which would avoid problems encountered by previous investigators. We only studied the work of experienced analysts and only used highly experienced analysts as raters for our initial studies. We tried to choose central, unambiguous, experience-near process features of both patient and analyst, and defined our variables in the language of the clinical surface.
Five of us are full-time practitioners, each with more than thirty-five years of clinical experience and Dr. Crouse is an experienced social scientist who has played a central role in evaluating our data. Our other directors are younger members with a special interest in research. We aimed at studying the nature of analytic interventions, the nature of the patient’s contributions, and the relationships and interactions between them. We tried to use methods which would avoid problems encountered by previous investigators. We only studied the work of experienced analysts and only used highly experienced analysts as raters for our initial studies. We tried to choose central, unambiguous, experience-near process features of both patient and analyst, and defined our variables in the language of the clinical surface.
From early in the project, the study of recorded psychoanalytic sessions ![]() led to sufficient clinical agreement among us that we were able to start developing scales for assessing the contributions of patient and analyst to the analytic work. We found that if we evaluated one session without understanding its context, our views were as discrepant from one another as reported by Seitz in his classical paper (1966) or Vaughan and coworkers (1997). However, we discovered that if we listened to two or three sessions immediately preceding the one to be rated, to establish a better understanding of how the patient-analyst pair was working together, we found our views converging, which in turn served as the basis for developing reliable ratings of central clinical variables.
led to sufficient clinical agreement among us that we were able to start developing scales for assessing the contributions of patient and analyst to the analytic work. We found that if we evaluated one session without understanding its context, our views were as discrepant from one another as reported by Seitz in his classical paper (1966) or Vaughan and coworkers (1997). However, we discovered that if we listened to two or three sessions immediately preceding the one to be rated, to establish a better understanding of how the patient-analyst pair was working together, we found our views converging, which in turn served as the basis for developing reliable ratings of central clinical variables.
In addition to clinical experience and theory, we drew upon previous psychoanalytic and psychotherapy research to formulate variables for the Analytic Process Scales. These include the Psychodynamic Intervention Rating Scale or PIRS (Cooper & Bond 1998; Milbrath et al. 1999), the Vanderbilt Psychotherapy Process Scales or VPPS (O’Malley, Suh and Strupp 1983), the Therapist Verbal Intervention Inventory or TVII (Koenigsberg et al,1988, 1993), and the Psychotherapy Process Q-Set (Jones and Windholz 1990). We were also influenced as time went on by our exposure to the Adult Attachment Interview (AAI) and the conceptualizations of the linguist Grice (1975) as cited by Main (1996), particularly the four characteristics of coherent and collaborative discourse in persons manifesting secure attachment. Such discourse “adheres to four maxims: quality (be truthful, and have evidence for what you say”), quantity (“be succinct, yet complete”), relation (“be relevant or perspicacious”) and manner (“be clear and orderly”). (Main, p. 240). We were also familiar with Bucci’s four somewhat overlapping features as components of Computerized Referential Activity (CRA), the degree to which speech was clear, concrete, specific and containing images (1997, p. 167).
Dividing a Session into Clinically Meaningful Segments, rated by the APS variables
The long process of devising variables, testing them on fresh recorded material, and repeatedly revising them, led to the development of eighteen variables assessing each analyst’s contribution and fourteen assessing that of each patient, selected to track elements central to analysis and psychodynamic therapy for the patient and the therapist as they vary during the course of each session. ![]() To accomplish this we developed a reliable procedure for segmenting sessions into psychoanalytically meaningful units for rating, permitting us to study the impact of one participant on the other as each session unfolds. Our procedure for segmenting was a modification of that described by Stinson, et al. (1994).
To accomplish this we developed a reliable procedure for segmenting sessions into psychoanalytically meaningful units for rating, permitting us to study the impact of one participant on the other as each session unfolds. Our procedure for segmenting was a modification of that described by Stinson, et al. (1994).
The segmenting of each session is fundamental to understanding the results reported here, because we are then able to estimate the impact of one participant upon the other in an unfolding way. Essentially all speech by each participant is contained within a segment, and segments are usually either patient segments, or therapist segments. The division into segments is often at the point of a change in speaker resulting in analyst segments and patient segments. When there is a rapid exchange between patient and analyst a segment may include several changes of speaker and is rated for both analyst and patient variables. The interaction between analyst and patient is studied by looking at the relationships between the patient and analyst variables studied over time. The segmenting procedure usually leads to about 8 to 30 segments per session, and each segment is rated on the clinical variables applying to that segment. Further details including data documenting the excellent reliability of the procedure in our hands are reported in Waldron et al. 2003.
The APS Coding Manual
The APS Coding Manual (Scharf, Waldron, Firestein, Goldberger & Burton 1999-2003, 80 pages) defines and illustrates each variable to be rated. Brief clinical examples illustrate ratings at the “0”, “2”, and “4” levels; the intermediate levels “1″ and “3″ are left to the judgment of the rater. Each example is designed to be easy to read and remember. In the course of years of examining scoring differences among our group members, we have refined our illustrations and instructions to raters. Our inter-rater reliability has steadily improved and we have now achieved a satisfactory level on virtually all our variables. Moreover, we have found that analysts need only brief training to achieve reliability using the manual. Full reliability scores with both senior and junior clinicians are reported in Waldron et al.(2003). As little as one rating hour has sufficed for training, followed by a discussion with a senior investigator, during which the new rater’s scores are compared with those of senior raters. We have found comparable levels of reliability for junior clinicians, after a series of meetings with our investigators to discuss interventions and patient response. In the data we have presented here, each APS score is the mean of the scores of four trained raters. ![]()
In the current study, the central patient variable studied in relation to the analyst variables was patient productivity, measured as progress either in response to the analyst’s intervention, or from the patient’s own momentum. Raters were instructed to score a segment “0” when they could find progress neither in understanding, nor in the involvement or collaboration in the analysis, nor in the nature of other developing emotional responses; “2” when there was moderate progress in the depth and breadth of understanding, or in emotional involvement and collaboration in the analysis, or in the nature of other emotional expressions; “4” when the patient made strong progress. Each of these points on the scale is illustrated with clinical examples (see Appendix 2 for coding manual definition and examples of this variable). The patient’s productivity immediately following each rated analyst intervention provided the central outcome variable (dependent variable) in this study.
The analyst variables fall into three clusters. The first, intervention quality, comprises two variables: one measures how well the analyst follows the patient’s productions, and the other measures the overall quality of the intervention. ![]() The second cluster, core analytic activities, measures the degree to which the analyst clarifies, interprets, and focuses on resistance, transference, and conflict. The third cluster, affective involvement, measures how much the analyst is confrontational and expressive of feeling.
The second cluster, core analytic activities, measures the degree to which the analyst clarifies, interprets, and focuses on resistance, transference, and conflict. The third cluster, affective involvement, measures how much the analyst is confrontational and expressive of feeling.
Intervention quality averages the ratings of the following two variables:
1. Following the patient assesses the degree to which an intervention follows the analytic surface by focusing on the patient’s most experience-near issues. It often determines the success of the analyst’s effort to communicate with the patient. For example, to what degree does the analyst follow meaningful affects (including the special negative affects such as anxiety, guilt, or low self-regard) and the patient’s moment-to-moment defenses.
2. Good intervention is a more global rating of the aptness of the type of intervention, the usefulness of its content, and the skill of presentation, including tact, timing and language appeal. Those readers interested in understanding in more detail our Coding Manual definition of good intervention with examples to illustrate scale points may review it in Appendix 2.
For the second cluster, core analytic activities, we assess five items: clarification, interpretation, and their major aims: addressing defense, transference, and conflicts. The raters estimate the degree to which each of these analytic activities is present, specifically disregarding the aptness or skill with which they are employed. Each of these elements is rated independently of the others, so that, for example, a given intervention could be rated “4″ for clarification, “2″ for interpretation, and “0″ for addressing transference.
1. Clarification is rated by the degree to which attention is called to insufficiently noticed surface features and how they may be psychologically connected.
2. Interpretation is rated according to how well the analyst’s intervention aims at transforming meaning by bringing aspects outside of awareness into full awareness.
3. Addressing resistance (or defenses operative in the session) is rated as the degree of focus on any measure the patient takes to avoid experiencing objectionable impulses, affects, thoughts, or fantasies. A psychological feature performing a defensive function may simultaneously serve drive, moral, or adaptive purposes. To be scored, addressing resistance must be manifest or, if inferred, easily identifiable by the rater and most analysts. Raters score the apparent aim of the intervention, not whether they agree with the analyst or therapist that defenses are present in the patient’s communication or the skill with which they are addressed.
4. Addressing transference is rated by the degree to which the patient’s reactions to the analyst or to the analytic situation are pointed out. The score increases with the amount of complexity and detail, which may include prior similar responses to the analyst or other persons.
5. Addressing conflicts is rated by the degree to which the analyst focuses on the patient’s conflicts in the segment—impulses or affects and their feared consequences or resulting moral concerns–and the connections between any of these, including related fantasies and memories.
The third cluster, analyst’s affective involvement, is assessed by averaging the following two variables:
1. Confrontation is rated by the degree to which the intervention introduces a special emphasis, urgency, or reiteration to point out that the patient is denying, avoiding, or minimizing an issue at the psychic surface. Raters are to disregard whether the confrontation seems constructive or harmful and score only for emphasis and urgency. The confrontational aspects of an intervention may be conveyed by tone of voice as well as content, making it essential to listen to a recording.
2. The contribution of the analyst’s feelings rates the degree to which voice quality and verbal content convey the analyst’s emotions, regardless of whether such emotional expression seems to encourage or interfere with the analytic work.
Encouragement of elaboration is separate from the three analytic intervention clusters and refers to the analyst’s request that the patient expand on what he or she has been relating. The request may be general (“Can you tell me more about that?”) or specific (“What comes to mind about the car emerging from underwater in the dream?”).
The patients studied
This report is based upon the study of three treatments, with three different analysts. These were studied initially to facilitate developing our scales, providing different treatment approaches and levels of clinical work. From perusal of several hours from each case, we estimated clinically that one patient had done relatively well; another appeared to be deadlocked after 660 sessions; and the third was chosen as a good representative analytic process. Although we make no claim that the sample is representative of all analyses, there were no systematic biases in selecting the sample, except that only patients who had agreed to be audiotaped could be included. The cases were chosen as a matter of convenience, to provide us with material for developing our APS. The sessions for the first two cases were chosen from the very beginning, the middle, and a few weeks before the end of the treatment, with no other selection criteria except that the sessions be from a complete week of analytic work. The first case was chosen because it was already transcribed, and the second because it was from a different analyst than the first. The third case, by yet another analyst, was chosen to extend the sample for purposes of further refining our instrument. The cases are briefly summarized elsewhere (Waldron et al. 2003). The sessions from this case were the only ones available, and came from the very end of that treatment. These were the only sessions rated using the APS; no other sessions were excluded from the sample. The data come from recorded sessions drawn from the 18 cases then in the collection of the Psychoanalytic Research Consortium (Waldron, 1998). ![]()
The Raters and their Training
The raters in the initial study were all experienced analysts (>35 years), trained at analytic institutes where the so-called American ego psychological viewpoint tended to predominate. Of course, their points of view about clinical work had altered through the experience of many years since training. These raters had participated variably in the development of the instrument, developing a degree of shared understanding about the variables. However, all ratings of each of the sessions in the study were independent, that is, raters did not discuss amongst themselves their views of the particular session rated until after ratings were completed, nor were they privy to the case summary provided above. Raters also did not know what followed each segment of the session at the time they rated that segment, and were not permitted to change ratings retrospectively.
The purpose of the replication study was to determine whether the relationship found in the initial study between intervention quality and patient productivity, reported later in this paper, would also be found if patient productivity were assessed by psychology interns who were blinded to the analysts’ interventions during the session to be rated. These interns had applied to the Karen Horney Clinic for internship, because of its reputation for teaching psychodynamic psychotherapy, which was a particular interest for each of them. The training and data collection with the Horney interns was as follows: Dr. Winarick, the training director, met with the interns as part of their regular academic experience for several weeks to familiarize them with the APS coding manual, a seventy-eight page document which defines and illustrates the thirty-two analyst and patient variables which constitute the APS. Following this initial familiarization, the interns were trained on a sample session in the use of the APS. Then, the interns read and listened to two complete sessions immediately prior to the session to be rated, to establish context (the same procedure as the original senior raters). Then they rated separately one of the nine sessions studied, on the APS variables assessing patient functioning (the analyst remarks being deleted), e-mailing their scores to Waldron. Waldron prepared a print-out each time, showing the four raters’ scores on each variable along with the average score of the four senior raters for each segment and variable. These print-outs were studied and discussed in detail in meetings among the interns and Drs. Waldron and Winarick. In order to sustain interns’ interest and sense of continuity, the senior investigators read to them the actual interventions as the session was reviewed, which had been omitted while they accomplished their ratings. The discussions tended to be lively and the students appeared to become engaged in the process of clarifying their own thinking about the treatments, leading to a sustained sense of involvement, despite their being blind at the time of the rating to the analyst’s remarks.
Statistical Analysis of the Data
The APS variables were chosen and defined to produce measurable differences between scores on each variable. These scores constitute the basic data of this study. Our statistical approach developed with ongoing consultations with Patrick Shrout, a statistician instrumental with others (Shrout and Fliess, 1979) in developing the intra-class correlation coefficient (used in this study). We also became aware of the utility of the multiple regression procedure when James Crouse, a professor of sociology and educational studies, joined our group. We check for relationships between the clusters of analyst intervention data and patient productivity scores. We also check for consistency of relationships between the individual analyst variables and patient productivity scores, to ensure that individual patterns are not being lost or concealed by aggregating the variables. Then by the method of partial correlation we hold constant the effect of differing analyst-patient pairs, to determine that any relationship found between analyst variables and subsequent patient productivity is true when examining each analyst-patient pair individually. Finally, by the method of multiple regression analysis we hold constant the effects of the other variables in order to discover the contribution of each individual analyst intervention variable to immediate patient productivity. In the replication study, we use the senior analyst scores on analyst variables and the psychology interns’ scores on the patient variables, applying the same analyses as in the initial study.
In this study, we rated nine sessions from three psychoanalyses drawn from the collection of the Psychoanalytic Research Consortium (Waldron, 1998): four sessions were taken from early, middle and late in a 324-hour analysis, three were selected from early, middle and late in a 660-hour analysis, and two were drawn from the end of a 388-hour analysis. The nine sessions produced a total of 123 segments rated for the analyst variables, and 117 segments rated for patient productivity.
The data are arrayed to show analyst intervention scores in relation to the patient productivity scores from the immediately prior and the immediately subsequent patient segment. This permits us to follow events of the session from two reciprocal perspectives: how the analyst’s activity affects the patient’s work, and how the patient’s work facilitates the analyst’s activity. When the patient becomes more productive, the analyst may be able to make higher-quality remarks, demonstrate better core analytic activity, and become more involved, so that any increased productivity following an intervention might not only result from the intervention itself but from the patient’s productivity in the previous segment (as shown using similar measures in the Caston et al. study, 1986). Since subsequent patient productivity might reflect both the patient’s previous productivity and the analyst’s intervention, we assessed the relative influence of these two factors using the method of multiple regression.
RESULTS
We report here the results based upon the ratings of the senior analysts, with replications for certain central findings based upon patient productivity scores generated by the Karen Horney Clinic psychology interns, who were blinded to analyst interventions. In our first paper applying the APS (Waldron et al. 2003) we found differences between the analytic activities of the three analysts, differences in the patients’ functioning within the session, and differences in the interaction between analyst and patient. In this paper we will focus particularly on findings related to ratings of quality of interventions.
 Figure 1 reveals the considerable variation in quality of intervention within each analysis, as well as substantial differences between them. [The 4 figures referred to are to be found following the references.] We have arranged the quality scores along the horizontal axis, increasing: from either 0 or 1 (the lowest level of quality) to the level of 3 or 4 (the highest levels). For each of the three patients the percentage of segment scores at each level of intervention quality is charted on the vertical axis. Inspection shows that 30% of interventions scored below 1, 64% between 1 and 3, and only 6% either 3 or 4. The striking differences among the patient-analyst pairs document the clinical impressions derived from reading the clinical summaries of the cases. For example, more than three-quarters of the segment scores for intervention quality for the case V4, a case viewed as problematic by the raters, fall below 1.
Figure 1 reveals the considerable variation in quality of intervention within each analysis, as well as substantial differences between them. [The 4 figures referred to are to be found following the references.] We have arranged the quality scores along the horizontal axis, increasing: from either 0 or 1 (the lowest level of quality) to the level of 3 or 4 (the highest levels). For each of the three patients the percentage of segment scores at each level of intervention quality is charted on the vertical axis. Inspection shows that 30% of interventions scored below 1, 64% between 1 and 3, and only 6% either 3 or 4. The striking differences among the patient-analyst pairs document the clinical impressions derived from reading the clinical summaries of the cases. For example, more than three-quarters of the segment scores for intervention quality for the case V4, a case viewed as problematic by the raters, fall below 1.
 In the two cases viewed clinically as more successful, only 7 and 8% respectively of interventions were scored 3 to 4, while the seemingly unsuccessful case, V4, had no interventions at these levels. It is possible that high quality interventions predict benefit even when they constitute a relatively low percentage of the total. However, a much larger sample will be necessary to examine the relationship between successful treatment and infrequent but very high quality interventions.
In the two cases viewed clinically as more successful, only 7 and 8% respectively of interventions were scored 3 to 4, while the seemingly unsuccessful case, V4, had no interventions at these levels. It is possible that high quality interventions predict benefit even when they constitute a relatively low percentage of the total. However, a much larger sample will be necessary to examine the relationship between successful treatment and infrequent but very high quality interventions.
The percent of segments falling at different levels of patient productivity is graphed for each patient separately in Figure 2, in a way similar to that of figure 1. The congruity of the curves of Figures 1 and 2 may demonstrate the mutual influence of patient and analyst, and suggests that each participant may not be able to achieve a high level of work without the other also doing so.
We now consider the relationships between the core analytic activities utilized by the analysts, the quality of these interventions, and the patients’ responses in the next patient segment in the three treatments. (The correlation matrices may be found in Appendix 1, Table 1, and the column and row numbers below refer to this table). One potential problem in studying the correlations between these variables is that a correlation found could be due only to differences between patient-analyst pairs, and not changes in productivity due to specific interventions. For example, such a spuriously strong correlation could appear if both analyst quality and patient productivity were high consistently for one patient-analyst pair, medium for a second patient-analyst pair and consistently low for a third analyst-patient pair. To protect against such misleading results, we used the statistical procedure called partial correlation, which holds the influence of patient-analyst pair constant. When we calculate the partial correlation of the mean core analytic activity (averaging the level of clarification, interpretation, analysis of resistance, transference and conflict together for each segment) with patient productivity in the next segment, there is a modest but significant correlation of 0.25 (row 3, column 1). Among the partial correlations of each individual core analytic activity with patient productivity, only analyzing resistance (r = 0.22, row 6, column 1) and analyzing conflict (r = 0.37, row 8, column 1) are significantly related to subsequent productivity. The reader will recall that these assessments of core analytic activities are made without considering the quality of the intervention, which is rated separately.
Continuing an examination of the results of our partial correlation procedure holding patient-analyst pair constant, we find intervention quality to be moderately correlated with next patient productivity (r = 0.44, row 2, column 1). Also, previous patient productivity has an important influence on the intervention quality that follows (r = 0.43, row 9 column 2), which illustrates how much the analyst’s work may depend on the patient’s contribution. Finally, subsequent patient productivity is related to previous patient productivity (r = 0.49, row 9, column 1), showing that the patient’s work has its own momentum as well. We have therefore found that the quality of the interventions is more strongly correlated with patient response than the core analytic activities combined or examined singly. In Figure 3 we have demonstrated in another way the degree to which quality analytic interventions are related to patient productivity by graphing the analyst’s intervention against the patient’s response. For each of these three analyses, the points are clustered along the straight line shown, and the relationship between the two variables is directly proportional. ![]() This relationship is found for each analyst’s interventions compared to that patient’s immediate next segment, indicating a consistent relationship between quality and productivity for each of our three cases, in this sample.
This relationship is found for each analyst’s interventions compared to that patient’s immediate next segment, indicating a consistent relationship between quality and productivity for each of our three cases, in this sample.
Note the absence of markers in the upper left quadrant of this chart If these patients were sometimes successfully carrying on their own analyses with little help from their analysts, we would find a number of markers in this area. Similarly, the lower right is virtually empty, indicating that there were no very high quality interventions followed by an absence of productive work.
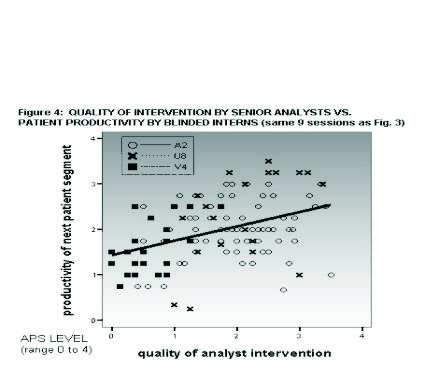
Figure 4 represents the same comparison as figure 3, except that the scores on patient productivity are those of the psychology interns who were blinded to the interventions of that session. The relationship between intervention quality as judged by the senior analysts and patient productivity as judged by the blinded interns continues to be significant, as can be seen for each patient separately on the scatterplot diagram ![]() . Thus a bias on the part of the senior raters in favor of patient responses to interventions these raters favored does not account for our findings.
. Thus a bias on the part of the senior raters in favor of patient responses to interventions these raters favored does not account for our findings.
Statistical multiple regression analysis was applied to examine which elements in the analysts’ interventions were most strongly associated with subsequent patient productivity (Appendix 1, Table 2 equations 1 through 9). Multiple regression is a procedure which tests the degree of association between what are called independent variables and a variable which is hypothesized to be perhaps dependent on these other variables. In this study, patient productivity in the next patient segment following an analyst segment was the dependent variable, and we measured the association between this productivity and five APS variables, or clusters of variables.
 We have already described the correlations of 1) core analytic activities and 2) the quality of the interventions with patient productivity. We also measured 3) the degree of the analyst’s involvement in each segment (by averaging the degree of confrontation and the degree to which the analyst shows feelings that contribute to or shape the intervention in the segment), and 4) how much encouragement of elaboration has occurred in the segment. Finally, we measured 5) previous patient productivity. These five independent variables were entered into a multiple regression procedure which determined how much each variable was associated with subsequent patient productivity when the other four independent variables are held constant statistically (Appendix 1, Table 2).
We have already described the correlations of 1) core analytic activities and 2) the quality of the interventions with patient productivity. We also measured 3) the degree of the analyst’s involvement in each segment (by averaging the degree of confrontation and the degree to which the analyst shows feelings that contribute to or shape the intervention in the segment), and 4) how much encouragement of elaboration has occurred in the segment. Finally, we measured 5) previous patient productivity. These five independent variables were entered into a multiple regression procedure which determined how much each variable was associated with subsequent patient productivity when the other four independent variables are held constant statistically (Appendix 1, Table 2).
The results show that, among the four predictor variables derived from the analyst’s activity, only the quality of intervention has a strong association with subsequent patient productivity when the other variables are held constant. Each one-point increase in intervention quality is associated with an average increase of six-tenths-of-a-point in subsequent patient productivity (B of .619 in Appendix 1, Table 2, equation 2, and a correlation [beta] of 0.59), a clinically significant effect ![]() . This strong relationship between quality of intervention and patient productivity is the central finding of this paper.
. This strong relationship between quality of intervention and patient productivity is the central finding of this paper.
To review, quality was assessed by averaging two variables with four major features–the degree that the intervention followed the patient’s immediate focus, was suitable in the type or blend of types of intervention, was apt in content, and was delivered with skill. Among the other analyst variables, only the core analytic activities proved importantly related to immediate patient productivity (B of .477, equation 4), and even this significant relationship is dependent on the quality of these interventions (the B drops to .037, a negligible value, in equation 5 when the quality of the intervention is held constant). ![]()
Thus the multiple regression analysis demonstrates that the averaged core analytic activities of clarification, interpretation, and the analysis of transference, resistance and of conflict, have a substantial correlation with immediate patient productivity, but only if they are carried out with high quality ![]() . The reader may well wonder whether the individual core analytic activities differ from one another in regard to the crucially important quality of the intervention. Further multiple regression analyses of the data showed that the quality of analytic work remained centrally important in affecting patient productivity for each of the five core analytic activities taken individually, just as it had for the five averaged together as shown in Table 2, Appendix 1.
. The reader may well wonder whether the individual core analytic activities differ from one another in regard to the crucially important quality of the intervention. Further multiple regression analyses of the data showed that the quality of analytic work remained centrally important in affecting patient productivity for each of the five core analytic activities taken individually, just as it had for the five averaged together as shown in Table 2, Appendix 1. ![]() So, in this preliminary study the quality of the analyst’s intervention, reflecting attunement to the patient, the choice of content and the aptness and skill of the intervention, was the analyst variable most strongly related to observed patient productivity in the ongoing therapeutic relationship, whether the intervention was predominantly an interpretation, or clarification and whether the analyst approached transference manifestations, defenses, or psychological conflict.
So, in this preliminary study the quality of the analyst’s intervention, reflecting attunement to the patient, the choice of content and the aptness and skill of the intervention, was the analyst variable most strongly related to observed patient productivity in the ongoing therapeutic relationship, whether the intervention was predominantly an interpretation, or clarification and whether the analyst approached transference manifestations, defenses, or psychological conflict. ![]()
We have also examined the degree to which the quality of the analyst’s intervention depends on the level of the patient’s productivity that preceded it. We would expect that, when a patient delves into matters of psychological importance, this productive process tends to develop momentum that carries over multiple segments. Such a pattern of relationship between current level and immediately prior level is quite typical of complex evolving phenomena sampled over time, such as the historic stock market. And indeed, as mentioned earlier, we found that prior segment patient productivity correlates both 0.60 with the analyst’s intervention quality, and 0.62 with subsequent segment patient productivity. Our multiple regression analysis allowed us to determine the relative contributions of intervention quality and prior patient productivity to immediately subsequent patient productivity (Appendix 1, Table 2, equation 3). We found that about half of the relationship between intervention quality and subsequent patient productivity was accounted for by the patient’s prior level of productivity: that is, when the patient had been more productive in the segment prior to the analyst’s intervention, the analyst made a higher quality intervention, and the patient continued to be more productive. But the other half of the relationship was a direct one between intervention quality and subsequent patient productivity, independent of prior patient productivity. This degree of direct relationship implies an important causal connection, unless another explanation for it emerges. ![]()
We next asked how much of the variation in patient productivity have we accounted for by our variables? It turns out that differences in analytic productivity across segments are only 46 % accounted for by the variables we have measured, together with the momentum of the process itself ![]() . Thus, despite the significant effect of intervention quality and prior patient productivity on later patient productivity, more than half of the differences in subsequent productivity remains unexplained by our variables. We believe this to be expectable in view of the complexity of the process we are assessing, and the often delayed impact of interventions.
. Thus, despite the significant effect of intervention quality and prior patient productivity on later patient productivity, more than half of the differences in subsequent productivity remains unexplained by our variables. We believe this to be expectable in view of the complexity of the process we are assessing, and the often delayed impact of interventions.
In view of the relationship found between the quality of intervention and immediate patient productivity, we must examine whether this could be accounted for by rater bias. Confirmation bias could incline our raters to find the productivity which they thought should follow a good intervention in the patients’ responses. Our replication study allows us to make a definitive test of confirmation bias, by re-calculating the regression analysis expressed in Appendix 1, Table 2. Recall that this analysis demonstrated that for each one-point increase in intervention quality, subsequent patient productivity increased six-tenths of a point. When we re-calculate this using patient productivity scores as rated by the blinded Horney raters, we find a less strong relationship, which is nevertheless statistically highly significant. Patient productivity increased by one-third of a point for every one point increase in intervention quality ![]() . This result further affirms a meaningful relationship in this sample between intervention quality and patient productivity.
. This result further affirms a meaningful relationship in this sample between intervention quality and patient productivity.
We also studied the relationship between scores for intervention quality and patient productivity of the next several segments following a given intervention, because our clinical experience led us to expect that the impact of an intervention may not become evident immediately. Indeed, the multiple regression for intervention quality and patient productivity continued to show a statistically significant relationship out to the fifth segment following a given intervention.
DISCUSSION
We report here the application of a newly published research tool for the investigation of psychoanalyses and psychodynamic therapies, the Analytic Process Scales (APS). The APS allows us to investigate psychoanalyses and psychotherapies by studying aspects of each case in a way that is both statistically reliable and clinically valid. The variables serve to delineate cases using central psychoanalytic concepts. We have demonstrated that experienced clinicians can agree on the nature and quality of interventions, once they are sufficiently familiar with a case. Because the APS assesses the nature and quality of interventions sequentially throughout an hour we have been able to examine their effects on subsequent patient productivity in the very next segment of the hour. The reliabilities we have achieved in assessing core psychoanalytic dimensions provide a basis for optimism about systematic studies of psychoanalytic process with suitable analytic data. The problems of achieving consensus in evaluating psychoanalytic treatments are not insurmountable, and can be resolved by methodological innovation and the participation of experienced clinicians (Seitz 1966; Rubovits-Seitz 1992; Caston et al. 1986, Caston 1993a; Caston and Martin 1993b).
We have discovered that the strongest analyst variable influencing patient productivity is the quality of the intervention that preceded it, rather than the specific type of intervention. This indicates, in our small sample of three patients and analysts, that attunement to the patient’s present state, the choice of an effective intervention, and its timing and tactfulness are most important to the progress of the analysis, rather than interpretation being necessarily more helpful than clarification, or analysis of transference necessarily more helpful than analyzing resistance etc. at that moment. The quality of the analyst’s contribution of any kind, so long as (s)he says “the right thing at the right time,” is the essential element. We do not dispute the major importance of interpretation, but with these three pairs we conclude that the other core analytic activities seem equally important, and that none is very effective unless of high quality.
A reader might gain the impression that we think there is only one “right thing” that can be said at any given time. In this respect, our title could be misleading. However, we tentatively believe that clinician judges are very aware of choices made in interventions, including tactfulness and timing of any given communication by analyst or therapist, and that it is these aspects which are reflected in the ratings of quality. Less idiomatically expressed, we do respect the impact of saying a right thing at a right time.
Most clinicians already assume the clinical truth of what we have found, but researchers have largely been unable to demonstrate the effects of differences in treatment approaches to patients, much less the impacts of differences in the quality of those approaches. Sequential analysis of the evolving contributions of patients and analysts or therapists provides a tool which can disentangle these varied contributions, as we have outlined in a recent paper (Crouse et al.2003).
We have been able to find strong evidence for the role of the patient’s previous productivity in facilitating the analyst’s making a high quality intervention. This empirically supports the contention that there is a complex interdependence in the dialogue between the analyst and patient. We have accounted for one-third of variations in patient productivity in the next segment, reflecting the varying quality of core analytic activities of the analyst and the patient’s own productivity in the previous segment. These constitute substantial findings, since psychoanalytic treatments are extremely complex emergent systems (Waldrop 1992; Kauffman 1995; Palombo 1999). Since the consequences of any intervention are multiple and often delayed in time, this degree of immediate relationship implies an important causal connection.
There are relevant findings from another similar study (Caston et al. 1986) in which the raters of patient response were blind to the interventions. Caston et al. used segments which were chosen on the basis of a coherent unit of patient material immediately following each intervention (ibid, 288), such as our patient segments. In that study one variable called insight (as defined in Appendix 18, 387-391) is approximately equivalent to our patient productivity variable. A separate group of judges rated the interpretiveness of the interventions, a measure which is approximately a blend of our variables for analyst clarifying and interpreting (see description of scale anchor points in appendix 14, 377-379). With blind judges they found a correlation between interpretiveness and insight of .30 (ibid, 291), similar to our findings (Table 2 above) of a .22 correlation of clarifications with productivity and a .26 correlation of interpretation with productivity. The Caston study eliminated possible bias which could stem from rater reaction to the prior analyst remarks, and provides a convergent line of evidence to support our findings.
Our findings show results that were not anticipated by the participating clinicians. The strongest held belief of this group of psychoanalyst raters at the outset of the study was that immediate patient productivity would be most enhanced by interventions rating at least moderately high for interpretation. Yet the correlation between the degree of interpretation and patient productivity was quite low (0.14 in Appendix 1, Table 1, when analyst-patient pair was held constant) and this relationship was no longer significant when the quality of interventions was held constant. One central requirement of a scientific procedure is that hypotheses can be disconfirmed by evidence (Grünbaum, 1984). and the APS is such a tool for disconfirming hypotheses about the variables of treatment process and their impact in different treatments.
A central method in applying the APS is respect for the need of clinician raters for a reasonably full context. This is supported by Rubovits-Seitz (1998). “[T]he anchor point for interpretations is not strictly empirical, but depends on a network of interdependent and continuously modifiable interpretations . . . [t]hus, there is no satisfactory way of interpreting a segment of clinical data in isolation from the contexts (including other interpretations) that precede and follow it …” (p. 213). Raters’ knowledge of both patient’s and analyst’s prior comments contributes to our study’s strength: we have achieved reliability on our clinical measures and can claim validity based upon careful attention by expert analyst judges to the meanings of the exchanges between patient and analyst, where context is indispensable. It should be noted that our psychoanalytic raters assessed the work in each segment without knowing what followed. We may then state that psychoanalytic interventions of quality lead to greater patient productivity in this small sample. That expert judges appear able to sense which interventions are likely to be beneficial to the patient in the short term probably reflects the impact of expert knowledge which may be difficult to verbalize, and is reminiscent of the burgeoning recent work on implicit memory and procedural knowledge. It could be said that the finding, if further replicated on wider samples, may lend further support to the value of clinical wisdom in conducting psychotherapy.
It may be asked why the relationships reported here have not emerged from earlier studies. In Reassessing Psychotherapy Research (1994) Russell provides a cogent discussion of the limitation of the previous approaches to assessing the relationships between intervention and benefit. For example, he shows how efforts to correlate the use of interpretation to patient benefit are bound to fail because the requirement of effective therapy is to make interventions attuned to the requirements of the patient at a particular moment in time. A well-attuned therapist will make very different interventions with any patient, depending on the patient’s needs and degree of resistance at the moment. This flexibility of technique cannot be measured using simple correlational research techniques, based upon simple hypotheses of what contributes to therapeutic benefit (Wampold 1997).
In contrast, the APS ratings, anchored by a manual with examples, reflect many of the complexities of clinical judgment in regard to interventions actually made by a treating analyst. We conclude that the only way to judge whether a given intervention is appropriate and helpful (high quality) is through the lens of psychoanalytic understanding. How widely this may obtain in the broad field of psychotherapies is a question awaiting further research.
What are the major limitations of this study?
1. We have not established, even preliminarily, whether high quality interventions are correlated with treatment outcome. The APS variables have a built-in potential to measure outcome when applied from early to late in treatment. Positive changes observed in patient functioning in the analytic situation from early to late in treatment are expected to reflect improved functioning in general, but the degree of relationship remains to be established. What is required are investigations of the relationship (or lack thereof) between a psychoanalytic or psychotherapeutic process characterized by frequent high quality communications from the therapist, and productive psychoanalytic work by the patient, and follow-up assessments of quality of life (Seligman 1995). Successful outcomes are the only “gold standard” for evaluating treatments.
2. It is clear that a clinical evaluation of psychoanalytic work, which is necessarily non-experimental in nature, can not rule out rival explanations of findings to the degree that may be achieved in some other areas of science (Rubovits-Seitz 1998). We would maintain that this does not invalidate the results, but gives reason for caution in generalizing from our findings. The heuristic value of the APS measures can only be determined by their ultimate utility in generating a pattern of useful findings.
3. The small size of our sample of 117 analyst interventions and patient responses from only three patient-analyst pairs limits the generalizability of the results. A larger sample of recorded analytic work from other analyst-patient pairs is required.
Our investigation of the quality of treatment may turn out to represent another way of examining elements addressed by the Boston Change Process Study Group researchers (CPSG: Stern et al. 1998, Nahum et al. 2002) studying change from the vantage point of the moment-to-moment interaction – what they call “the local level.” The emphasis of this group is upon the co-construction of the relationship, which they believe provides the opportunity for changes in “implicit relational knowing” – changes at a level which may correspond with Bucci’s “non-symbolic” and “nonverbal symbolic” levels of information processing (2000). The intricate detailing of how the analyst’s moment-to-moment response to the patient can facilitate such positive developments by participation with the patient is conveyed in an example from a child analysis (Nahum et al. 2002, pp.1054-5).
One consequence of these considerations is a proposed change in terminology. It has been customary to talk in terms of the analyst’s “interventions.” This term may not imply the subtle ongoing interaction, which can lead to special “moments of meeting”, and impacts the degree of “fittedness” between the two participants in treatment, terms used by the CPSG to describe important dimensions of treatment. The analyst’s contribution is certainly reflective of the analyst’s implicit relational knowledge, in regard to each moment with each patient. It seems to us preferable to describe the analyst’s contribution and the patient’s contribution, as more truly reflecting the complex interplay. We believe that our clinician raters are responding to this complex contribution in assessing the quality of the contribution of the analyst from moment to moment, and it is most likely because of its importance that we have found a strong relationship with the very next patient contribution.
REFERENCES
ABLON, S. and JONES, E. E. (1998). How expert clinicians’ prototypes of an ideal treatment correlate with outcome in psychodynamic and cognitive-behavioral therapy. Psychotherapy Research, 8: 71-83.
BORKOVEC, T. D. and MIRANDA, J. (1996). Between-Group Psychotherapy Outcome Research and Basic Science. Psychotherapy and Rehabilitation Research Bulletin, no. 5: 14-20.
BUCCI, W. (1997). Patterns of Discourse in “Good” and Troubled Hours: A Multiple code Interpretation. J. Amer. Psychoanal. Assn., 45:155-187.
BUCCI, W. (2000). The need for a “psychoanalytic psychology” in the cognitive science field. Psychoanalytic Psychology 17: 203-224.
CASTON, J., GOLDMAN, R.K. and MCCLURE, M.M.. (1986). The Immediate Effects of Psychoanalytic Interventions. In The psychoanalytic process: theory, clinical observations, and empirical research. Weiss, J., Sampson, H. and the Mt. Zion Psychotherapy Research Group. New York, Guilford, 277-298, 377-379, 387-391.
CASTON, J. (1993a) Can analysts agree? The problems of consensus and the psychoanalytic mannequin: I. A proposed solution. J. Amer. Psychoanal. Assn, 41:493-511.
CASTON, J. and MARTIN, E. (1993b). Can analysts agree? The problems of consensus and the psychoanalytic mannequin: II. Empirical tests.J. Amer. Psychoanal. Assn, 41:513-548.
COOPER, S. and Bond, M. (1998). The Psychodynamic Intervention Rating Scale. Unpublished.
CROUSE, J., BURTON, A., FIRESTEIN, S., SCHARF, R., & WALDRON, S. (2003). A path analytic strategy to analyze psychoanalytic treatment effects. Int. J. Psychoanal., 84:1263-1280.
DAHL, H. (1988). Frames of mind. In PsychoanalyticProcess Research Strategies, Dahl, H., Kächele, H., and Thomä, H. (eds.). New York: Springer-Verlag, 51-66.
DAHL, H. (1991). From the key to understanding change: emotions as appetitive wishes and beliefs about their fulfillment. In Emotion, Psychotherapy and Change, Safran, J. and Greenberg, L. (eds). New York: Guilford Press.
GARDUK, E. L. and HAGGARD, E. A. (1972). Immediate effects on patients of psychoanalytic interpretations. Psychological Issues, 7, monograph 28, 1-85.
GEDO, P.M., SCHAFFER, N. (1989). An Empirical Approach to Studying Psychoanalytic Process. Psychoanalytic Psychology, 6:277-291.
GLASS, L. L., KATZ, H. M., SCHNITZER, R. D., KNAPP, P. H., FRANK, A. F. and GUNDERSON, J. G. (1989). Psychotherapy of schizophrenia: an empirical investigation of the relationship of process to outcome. American Journal of Psychiatry, 146: 603-608.
GRICE, H.P. (1975). Logic and Conversation. In p. Cole and J.L. Moran (Eds.) Syntax and Semantics III: Speech Acts (pp. 41-58). New York. Academic Press.
GRUNBAUM, A. (1984). The Foundations of Psychoanalysis. Berkeley, University of California Press.
JONES, E. E. and WINDHOLZ, M. (1990). The psychoanalytic case study: toward a method for systematic inquiry. J. Amer. Psychoanal. Assn, 38: 985-1015.
JONES, E. E. and PULOS, S. M..(1993). Comparing the process in psychodynamic and cognitive-behavioral therapies. J. Consult. & Clin. Psychol., 61(2): 306-316.
KAUFFMAN, S. (1995). At Home in the Universe: the Search for Laws of Self Organization and Complexity. New York: Oxford University Press.
KOENIGSBERG, H., KERNBERG, O., ROCKLAND, L., et al. (1988). Developing an instrument for characterizing psychotherapy techniques in studies of the psychotherapy of borderline patients. In Psychoanalytic Process Research Strategies. ed. H. Dahl, H. Kächele, & H. Thomä. New York, Springer-Verlag, pp. 147-162.
KOENIGSBERG, H., KERNBERG, O., APPLEBAUM, A.H., & SMITH, T. (1993). A method for analyzing therapist interventions in the psychotherapy of borderline patients. J. Psychother.Practice & Research 2:119-134.
LUBORSKY, L., BACHRACH, H., GRAFF, H., PULVER, S.& CRITS-CHRISTOPH, P. Preconditions and Consequences of Transference Interpretations. J. Nerv. & Ment. Dis.: l67, 391-401.
LUBORSKY, L., CRITS-CRISTOPH, P., MINTZ, J., and AUERBACH, A. (1988). Who Will Benefit From Psychotherapy? Predicting Therapeutic Outcomes. New York: Basic Books.
LUBORSKY, L. and CRITS-CRISTOPH, P. (1998). Understanding Transference: the Core Conflictual Relationship Theme Method. Washington, The American Psychological Association.
MAIN, M. (1996) Introduction to the Special Section on Attachment and Psychopathology: 2. Overview of the Field of Attachment. J. Consult. & Clin. Psychol., 64: 237-243.
MALAN, D.H. (1976) The Frontier of Brief Psychotherapy: An Example of the Convergence of Research and Clinical Practice. New York & London, Plenum.
MILBRATH, C., BOND, M., COOPER, S., ZNOJ, H.J., HOROWITZ, M.J.& PERRY, J.C.(1999). Sequential Consequences of Therapists’ Interventions. J. Psychother. Pract. & Res., 8: 40-54.
NAHUM, J.P., for the The Boston Change Process Study Group (CPSG) Brushweiler-Stern, N., Harrison, A.M., Lyons-Ruth, K., Morgan, A.C., Nahum, J.P., Sander, L. W., Stern, D.N. & Tronick, E.Z. (2002). Explicating the implicit: The local level and the microprocess of change in the analytic situation. Int.J.Psychoanal., 83: 1051-1062.
NORVILLE, R., SAMPSON, H. and WEISS, J. (1996). Accurate interpretations and brief psychotherapy outcome. Psychother. Res., 6:16-29.
O’MALLEY, S.S., SUH, C.S. & STRUPP, H.H. (1983). The Vanderbilt Psychotherapy Process Scale: a Report on the Scale Development and a Process-Outcome Study. J. Consult. & Clin. Psychol.: 51, 581-586.
PALOMBO, S. R. (1999). The Emergent Ego: Complexity and Co-evolution in the Psychoanalytic Process. Madison, CT: I.U.P.
RUBOVITZ-SEITZ, P. (1992). Interpretive methodology: some problems, limitations, and remedial strategies. J. Amer. Psychoanal. Assn, 40:139-168.
RUBOVITS-SEITZ, P. (1998) Depth Psychological Understanding: The Methodological Grounding of Clinical Interpretations. The Analytic Press, Hillsdale, NJ and London
RUSSELL, R. L. (ed.) (1994). Reassessing Psychotherapy Research. New York: Guilford.
SEITZ, P. (1966). The consensus problem in psychoanalytic research. In Methods of Research in Psychotherapy. Gottschalk, L. and Auerbach, A. H. (eds.). New York: Appleton-Century-Crofts.
SCHARF, R. D., WALDRON, S., FIRESTEIN, S. K., GOLDBERGER, A., and BURTON, A. (1999). The analytic process scales (APS) Coding manual. Unpublished.
SELIGMAN, M. (1995). The effectiveness of psychotherapy: the consumer reports study. American Psychologist, 50: 965-974.
SHROUT, P.E. & FLEISS, J.L. (1979). Intraclass correlations: Uses in assessing rater reliability. Psychological Bulletin 86, 420-428
STERN, D.N., SANDER, L.W., NAHUM, J.P., HARRISON, A.M., LYONS-RUTH, K., MORGAN, A.C., BRUSCHWEILER-STERN, N. & TRONICK, E.Z. (1998). Non-interpretative mechanisms in psychoanalytic therapy: The ‘something more’ than interpretation. Int.J.Psychoanal., 79: 903-921.
STINSON C, MILBRATH C, REIDBORD S & BUCCI W (1994). Thematic segmentation of psychotherapy transcripts for convergent analyses. Psychotherapy 31: 36-48.
VAUGHAN S, SPITZER R, DAVIES M & ROOSE, S. (1997). The definition and assessment of analytic process: Can analysts agree? Int. J. Psycho-Anal., 78:959-973.
WALDRON, S. (1998). Description of the Psychoanalytic Research Consortium. http://www.psychoanalyticresearch.org, website.
WALDRON, S., SCHARF, R.D., HURST, D., FIRESTEIN, S.K., and BURTON, A. (2003) What Happens in a Psychoanalysis? A View through the Lens of the Analytic Process Scales (APS). In Press, Int.J.Psychoanal.
WALDROP, M. (1992). Complexity: The Emerging Science at the Edge of Order and Chaos. New York: Simon & Schuster.
WAMPOLD, B.E. (1997). Methodological problems in identifying efficacious psychotherapies. Psychother. Res., 7:21-43.
WEISS, J. & SAMPSON, H., & THE MT. ZION PSYCHOTHERAPY RESEARCH GROUP (eds.) (1986). The Psychoanalytic Process: Theory, Clinical Observation, and Empirical Research. New York: Guilford Press.

* Correlations are bolded if p < .05. Correlations in this table are Pearson correlations, which can range from -1.00 if the two variables are perfectly inversely related, to zero if there is no relationship, to +1.00 if there is a perfect positive correlation. Three standard correlations, above the diagonal, are no longer significant when controlling for analyst-patient pair: these three pairs of boxes are lightly shaded. Any correlation above .24 is significant at the .01 level or higher. N=117 for full correlations which included the patient productivity variables, and n=123 for analyst variables with each other. For the partial correlations, degrees of freedom equal 113.
table 2 goes here
Table 2: Regressions of Patient Productivity on Analyst Interventions and
Prior Patient Productivity: N = 117 Analyst Segments
With Complete Data on All Variables
* Designates “B” coefficients significant at p < .01
1. “Constant” represents the intercept of the slope on the y-axis. Since the y-axis represents the intervention, if a positive number it signifies that the patient has some productivity even when the analyst’s intervention is judged to have no value in the respect measured by each equation.
2. “Ad R2″ is an abbreviation for “adjusted R squared”. This number, part of the multiple regression formula output, represents the variance in the dependent variable (patient productivity) accounted for by the combination of independent variables in each particular equation.
3. “B” is the most important measure of the relationship between the dependent variable, patient productivity, and the independent variables listed. “B” is the change in patient productivity associated with a one-point increase in the variable, holding all other variables in the equation constant. Beta represents the standard deviation change in the dependent variable associated with a one standard deviation change in the independent variable while holding other variables constant. While included here because Beta is customarily reported in a regression analysis, it does not convey additional information in our study, because the “B” statistic serves this purpose fully when the measures being studied all have the same metric (in this case Likert-type scales with a range of from zero to four).
4. Beta represents the standard deviation change in the dependent variable associated with a one standard deviation change in the independent variable while holding other variables constant.
APPENDIX 2: SCORING OF PATIENT PRODUCTIVITY
WHAT IS THE DEGREE OF THE PATIENT’S OVERALL ANALYTIC
PRODUCTIVITY DURING THE SEGMENT?
This variable measures the patient’s overall psychoanalytic progress during the+ segment, whether occurring in response to the analyst’s intervention, or emerging from the patient’s independent momentum, or a mixture of the two.
Score according to the degree that, overall, progress is achieved during the segment in: the depth or breadth of the patient’s or rater’s understanding; and/or the intensity of the patient’s involvement and collaboration in the analysis; and/or the quality of other momentary emotional expressions. The score increases as there is more complexity or detail, and decreases as the patient’s expressions are less affectively meaningful, for instance when feelings are either suppressed or exaggerated.
Improved understanding includes more comprehension of any psychological features such as conflicts, fantasies, identifications, or self esteem.
Advances in the patient’s emotional involvement and collaboration in the analysis consist of better emotional expressiveness, self reflectiveness, or useful attention to the analyst’s focus.
Improvement in any other momentary emotional expressions is seen in headway with defenses, affects, inhibitions (for example of assertiveness), specific symptoms (for example obsessive doubting), or character symptoms (for example antagonism).
Score 0 when, overall, there is no analytic progress during the segment in understanding by the patient or rater, or the involvement or collaboration in the analysis, or the quality of other momentary emotional expressions.
Example: THE BUSINESSMAN AFRAID OF HIS FATHER
A man is undertaking analysis because his wife finds him removed and insensitive to her concerns, and has threatened to leave him. He works in a family business founded by his father, who thinks he is insufficiently capable to warrant major responsibilities. The patient begins with an indifferent tone, “There’s really nothing new, so I’m going to tell you the usual things . . It’s a month since the baby was born, and Sally (wife) is nervous because the nurse will finish this week . . (with more enthusiasm) The appliance line is selling pretty well, which is a surprise in this economy.”
Explanation: The patient begins by indicating his lack of emotional openness, and then ignores his emotions and those of his wife. There are no dimensions of analytic advance.
Score 2 when the patient, overall, shows moderate analytic progress during the segment in the depth and breadth of the patient’s or rater’s understanding, or the person’s emotional involvement and collaboration in the analysis, or the quality of other momentary emotional expressions, including inhibitions and symptoms. There is usually moderate complexity or detail.
Example: The patient, continues, “I was driving a company van yesterday, and a truck backed right into me. He took off like a bat, but I wasn’t going to let him get away from me. I drove after him, and got his license number! Back at the factory my father acted as if it was all my fault. I thought I handled it pretty well, but I can never win with that guy. A lot of time I end up feeling that he thinks I’m ineffective, and that he’s the great efficient operator.”
Explanation: During the segment, the patient shows a moderate understanding of his feelings of rivalry with his father, and the fugitive truck driver, as is seen in his reflections about his father’s depreciation and his feelings that he never wins. A time dimension is included, “A lot of time I end up feeling”. His emotional engagement, collaboration, and self reflectiveness are moderately improved, and there is moderate complexity and detail.
Score 4 when the patient, overall, makes strong analytic progress during the segment in the depth and breadth of the patient’s or rater’s understanding, or the person’s emotional involvement and collaboration in the analysis, or the nature of other momentary emotional expressions, including inhibitions and symptoms. There is usually strong complexity and detail, which may link current experiences, past experiences, and responses to the analyst.
Example: He continues, “I feel that my father doesn’t really want me to do better in the business, but I can’t be sure that it’s happening. Maybe I’m making it all up because I’m stressed out by the accident.” The analyst remarks, “At moments with strong emotional charge, like this one about your father, you become vague and indecisive so as to obscure feelings which frighten you”. The patient, “I can’t see that at all . . I guess I do stay away from confrontations with people, I can see that. Going against my father or the other people at work can be big trouble, so it’s better to just go along . . I don’t open my mouth much here with you either. You understand this stuff better than I ever could, and could make me look like a real jerk in about two seconds . . I really used to be afraid of my mother when I was a kid . . she screamed and strapped me all the time.”
Explanation: The patient responds to the analyst’s interpretation with moderate understanding of his passivity, and fear of his father and co-workers; and he expresses a similar fear of the analyst. He then recalls memories of his mother terrorizing him as a child. Although the patient has only moderate understanding of these experiences, his communications permit the rater to strongly comprehend the connections between the three sets of experiences, concerning his father, analyst, and mother. Emotional involvement, collaboration, and self reflectiveness are strong; and there is a high degree of complexity and detail.
APPENDIX 2 CONTINUED: SCORING OF GOOD INTERVENTION
TO WHAT DEGREE IS THIS A GOOD INTERVENTION?
This is a global variable that rates the overall quality of the intervention.
Rate the aptness of the intervention’s type, the potential usefulness of its content, and the skill of its presentation. The skill of the presentation is scored higher when the intervention is more tactful, well timed, and its language is more clear, vivid, or likely to appeal to the patient. The score also increases when the intervention is more direct or more relevantly complex and detailed. The length of the analyst’s contribution should not necessarily influence its score.
We divide interventions into four types: three distinctively analytic ones — encouraging elaboration, clarification, and interpretation — and those offering support, which include all other interventions.
There is, of course, more than one useful response to a patient’s material. The rater should evaluate the potential effectiveness of the intervention by following the analyst’s chosen direction, but should also consider how well the intervention approaches what you regard as optimal, with some thought as to what you would have done in the same situation. Be careful not to score inappropriately high by giving the analyst’s effort the “benefit of the doubt.”
Rate according to the highest level of the variable reached, even if the segment is long and most of it warrants a lower rating.
If an intervention seems useful but not remarkable, it is usually rated at 2 or less.
SCORE 0 when the type of intervention, or its content, or the skill of its presentation do not suit the patient’s expressions at all.
Example: The Man Whose Brother Entered a Cave
The patient is a vulnerable, self-defeating young man who is conflicted about expressing his anger and started analysis because of insufficient progress in his career. This session starts with the patient describing an evening with his parents and his younger brother, John, who has been visiting. “The dinner with my parents went all right. John and I walked past a beautiful church and I pointed out a carving on an arch. John seemed interested, but didn’t have much to say about it, so I started talking about work. The analyst said “You seem to have let your brother get the best of you.”
Explanation: Although the intervention applies to the patient generally, its content does not match the patient’s communications and it is insufficiently tactful.
SCORE 2 when the intervention is a moderately suitable response to the patient’s communications. The type or blend of types of intervention is at least reasonably apt, the content addresses the patient’s expressions in a potentially moderately useful way, and the presentation is reasonably tactful, well timed, and verbally appealing to the patient. There is a moderate degree of directness or relevant complexity.
If an intervention seems useful and reasonably well designed, but not remarkable, the rating is usually 2 or less.
Example: The patient continues “John wanted to know if he could stay at my apartment and then, out of the blue, he punched me on the arm so hard that it really hurt. Well . . . I mean! . . . I told him that he could stay with me last night, but not over the weekend. We’re inviting a lot of people to a party on Saturday.” The analyst intercedes “You speak about your brother punching you on the arm, and then continue as if that were quite usual. You seem to be avoiding getting angry at John.”
Explanation: This blend of clarification and interpretation is an apt type of intervention, which calls attention to the patient’s denial of his anger moderately well. There is reasonably suitable tact, timing, and verbal appeal, as well as moderate directness and complexity.
SCORE 4 when the intervention is a highly suitable response to the patient’s communications. The type or blend of types of intervention is very apt, the content focuses on the patient’s expressions in a potentially very effective way, and the presentation is usually very tactful, well timed, and uses clear and vivid language. There is usually a high degree of directness or strong relevant complexity, possibly linking current experiences with past experiences or experiences involving the analyst.
Example: The patient says “I had a dream last night. There were two holes in a barren rock and I was lying in one of them. I guess it means that I was dead, like in a grave . . . [sigh] . . . It reminds me of the time my family went on vacation when I was nine, and John and I found an opening in a rock face and he crawled in. The earth over the entrance started to slide, and my father ran over with a piece of wood and braced it. Dad turned to me white-faced and furious, and said ‘He could have died in there! How could you let him do that?’” The analyst says “Your father’s accusation touched on a deep feeling in you. John’s hitting you seems to have brought the accident and your father’s accusation back to your mind, that you would be willing to see John die. It’s as though you are guiltily saying, in your dream, ‘I’m the one who deserves to be in a rocky grave, not John.’ Feeling that you are capable of being so destructive leads you to back off from standing up for yourself with John and to feel pessimistic about yourself and about this treatment helping you.”
Explanation: The interpretation is an apt type of intervention, strongly calling attention to the punishment the patient feels he deserves for his past and present murderous impulses. The interpretation is sensitive, well timed, vivid, and dexterously expressed. Links between the patient’s recent conflicts and past experiences show considerable complexity. (For illustrative purposes, this intervention is given as if said all at once. Most likely such an intervention might best be given in a way that would give the patient an opportunity to respond to each part before proceeding to the next part of the intervention.)
END NOTES